
One of the many fractures I sustained in the wreck I survived, was my Scapula. It is rare to fracture the Scapula. In fact, I didn’t just fracture it……I shattered it.

I endured a continued loss of function in my right arm, one failed shoulder surgery attempt by a local Orthopedic Surgeon 10 months after initial injury; additional pain and continual loss of function, 2 years of excruciating and unrelenting pain in my right shoulder, right ribs, and back .
(It turns out that there are NOT many Orthopedic Surgeons who have actually been trained to rebuild a Scapula and specialize in its reconstruction. We also learned that just because someone is an Orthopedic Surgeon or a Trauma Surgeon does not mean that they are able to repair ALL orthopedic fractures.)
My family and I did a ton research and read so many articles, studies, and eventually ended up having to go out of State to get my Scapula repaired. I was referred to an Orthopedic Surgeon who specialized and had a special niche with Scapula repair. In fact, he runs the Scapula Institute out of St. Paul, Minnesota (in partnership with Regions Hospital and Health Partners) and accepts referrals from around the World.
When I went to Minnesota, the first test I received was an EMG, x-rays, and then a CT Scan. I learned that due to the delayed treatment of my shoulder injury, I had developed Suprascapular Nerve Palsy (nerve damage). There was no guarantee this would not remain permanent – even after surgery repair.
This page is my way of telling my Scapula story and hopefully providing some educational information to potential patients, providers, and the public at large. If you have a Scapula fracture – this is the place you want to be!!! The Surgeon is Dr. Peter Cole, MD from Regions Hospital in St. Paul, Minnesota. He is also affiliated with The Scapula Institute.
It is important to understand that most scapular fractures are handled non-operatively. That being said, if surgery is required, not all scapula fractures are repairable. One thing I loved about Dr. Cole is that he is straight up about this up front. He said he could not guarantee 100% relief of my pain or 100% mobility – however, he felt that after looking at all my previous scans (we had mailed all these records to him prior to him taking my case) that he could reduce the majority of my pain and restore a good portion of my mobility.
I want to stress that it is also important to know how to advocate for yourself if there is hope that a repair can be made. In today’s world of progressive medicine. It is highly likely that this may be a very real possibility. If I would have just “accepted” the words from the many surgeons I went to for consultation of repair
-
“nothing can be done”
-
“your scapula cannot be repaired”
-
“you will just have to live with this disability and pain for life”
-
“there are no orthopedic surgeons that work on scapulas/shoulderblades”
-
“stop malingering your shoulder pain isn’t real it should be healed by now”
-
“you will most likely lose the use of your arm eventually”
-
“I cannot explain why you are still having trouble gripping or lifting your arm and moving your shoulder”
-
” I agree it shouldn’t be crunching like that (crepitus) but it just takes time to heal”
-
“you just need to accept your limitations”
-
“we don’t pay for providers out of network or out of State” (from insurance company)
-
“if all these surgeons in Michigan say it cannot be repaired what makes you think the surgeon out of state can fix it” (from insurance company)
-
“if the first surgery didn’t fix it, it can’t be fixed” (from insurance company)
-
“the IME Dr. said all your bones are healed and you are ready to return to work with no limitations” (from insurance company before reconstructive surgeries)
and my all time favorite line from most providers when they don’t know what else to tell you….
-
“if you lose weight your shoulder will feel better and the pain will go away”
This page is just one aspect of my orthopedic story. I have attempted to include both basic and technical information. If you are interested in more detailed information, please contact me directly. I am glad to share what I can.
My orthopedic scapula and torso surgeries consisted of the following:
2014 – Scapula Modified Judet Approach ORIF surgery in Michigan, no plating or reconstruction done – even though this was the original surgery plan. Rib Plating surgery done during same surgery time.
2016 – Two surgeries done in January at Regions Hospital in St. Paul, Minnesota. The first one was to lay antibiotic beads to prep the area for reconstruction. We waited 5 days and then the second surgery was done. This was to actually do the reconstruction with a bone graft from the pelvis. This ended up being altered due to a large amount of Heterotopic Ossification in my shoulder (excess bone formed where it shouldn’t be) that was cut up, ground up, and used along with cadaver bone, to create a “compound” instead. This was amazing because we didn’t have to use the pelvis to get bone from. I was home within 2 weeks. I had 3 stainless steel plates and a multitude of stainless steel screws/nails added to my bionic collection (along with my rib plating from 2014). I felt almost instant relief all around the shoulder in regards to pain once I woke up in recovery. I mean – I had the surgery pain, but this was very different. It was an immediate noticeable difference.

Approximately 2 weeks after the surgeries, I had completed a physical therapy session at my home. I was lifting my right arm gently as I was getting help getting dressed by my husband. I heard a LOUD pop and felt enormous earth shattering pain shoot up to my neck and through my shoulder. I was instantly in tears. I went to my Primary Care Provider. She could feel no breaks. However, she contacted Dr. Cole (as did I) and let him know about the “pop and pain”. I was going back to Minnesota in a few days already, for a scheduled appointment, and to save my body from too much radiation my PCP at the time opted for me to wait until I was in Minnesota to get examined Radiologically.
In Minnesota, the very next week, we discovered my Acromion was fractured. Dr. Cole stated that when there is delayed treatment of an injury (and mine had been delayed for over 2 years), sometimes when it is put back into a proper position that this can cause stress on the other bones and sometimes they can break. We didn’t know what an Acromion was, so we researched that too. After 3 months of very conservative treatment, that fracture was stubborn and would not heal. In fact it started developing a gap. The pain was ridiculous. So after another exam in May, a surgery was scheduled on May 5, 2016 (the same day) to plate the Acromion.
2016 – Surgery to add stainless steel plates and stainless steel screws to the Acromion nonunion fracture to stabilize the area. I was there for a few days after that for recovery and follow through. 
Since the surgeries I can tell you that I have regained the majority of the use (mobility) of my right arm and hand. I don’t have the same strength I used to have before the wreck, but that is continually improving as time goes on with physical therapy and sheer personal grit. The surgeries also got rid of almost all of the pain in the shoulder/scapula. This alone, to reduce the pain, made it completely worth it.
I still have some hot spots of pain or “electrical shocks” that happen in my scapula/shoulder area. I still have the nerve damage which may or may not heal over time. I am very grateful however – I can hug my kids again and use my arm and I am eternally grateful to Dr. Cole and his whole Trauma team for believing in me and in their own skills as well.
I realize I may never get back to 100% like I was before the wreck. However, I am working hard to get as close as I can.
2018 – I am still seeing improvement in my shoulder and arm strength and mobility as time progresses. I do notice a bit of tiring with over the head work, lifting, and prolonged raising of the arm is a bit tiring. The posterior portion of the should has a bit of resistance feeling to it. I am not sure if this is because of the plates that are in place or just a constant muscular contraction/spasm that is more annoying than it is debilitating. When in the shower, I just prop my right elbow up against the wall when washing my armpit so my arm doesn’t tire of being held up. However, this is a negligible inconvenience and is not accompanied by pain, so I am grateful still the same.
2021 – I am thrilled to be able to add this update about my scapula and shoulder to this page. I have nearly full range of motion (ROM) with my right arm now. I still struggle sometimes with a couple of minor mobility resistance issues, various sensation alterations which are inconsistent in presentation, and the occasional “flare of surprise” (random pain jolts). Though I am free from daily pain in the scapula region, I do still get a sense of “pressure” or “fullness” on that side of my body. Some things that are consistently inconsistent as they continue are
- lifting arm up middle of back offers a bit of resistance and lack of archability up the center of my back – though only slightly more difficult than good left arm
- no lack of strength with adduction (towards the body), equal strength with left side of body with abduction (away from the body) laterally (sideways).
- can lift both arms up equally at the same height, though the right arm still gets shaky and a sense of resistance posteriorly and at the tip of the shoulder seem to be an unchanged constant, along with an increased intolerance of being able to hold the arm up for very long.
- occasional pins and needles (that asleep feeling) in the entire palm occasionally – I usually just end up massaging it out or stopping whatever activity appears to be causing it to get exacerbated.
- I can “chicken-wing” my elbow up only slightly lower than my left side while feeling a bit of resistance or pressure on top of shoulder – though does not stop me from completing the movement.
- When I have done a lot with my hands or arms (lifting, pushing, pulling, etc) I do benefit from resting my elbow on a wall when washing my armpit, shaving, or putting on deodorant, This is truly day specific as some days I can do these things without propping my elbow (as long as I do if fairly quickly).
- I have trouble twisting to reach my butt with my right hand as I just am not able to reach that far, so I use my left hand for all the personal hygiene (good thing I am left handed I guess). I am not sure this is totally related to the shoulder though. I am curious if my rib plating prevents me from getting that twist going that is needed for that action.
Every once in a while I get a whole shoulder ache and deep pain radiating across the whole body of the scapula and up to the neck…mostly directly around the scapula itself though when this does happen. When this first happened it scared the crap out of me because I was concerned about going backwards in my recovery. I even called the Clinic all freaked out about it. It eventually resolved on its own and I am still unsure why it went crazy like that as no particular activity could be traced to it. It lasted for nearly a week to a week and a half. I was so relieved when it calmed back down. Overall though, I am still extremely happy and confident with the healing of my shoulder/scapula region since my surgeries. I am so very grateful still for nearly all of the mobility I have gained and need to function – at least from an orthopedic standpoint. I would highly recommend the procedures I had done to anyone out there suffering and potentially losing function.
If you want to know more about this just email me HERE
The picture here below is a picture of the Trauma Team getting geared up for a surgery at Regions Hospital.

Now to the fun stuff. You know I cannot resist the details when it comes to sharing the educational baton….below is a compiled very short list of some basic information. Hopefully this helps you if looking for information about the Anatomy of Shoulder Injuries, Scapular Fractures, or Acromion Fractures.

THE ANATOMICAL SHOULDER
The shoulder is an elegant and complex piece of machinery. Its design allows us to reach and use our hands in many different positions. However, while the shoulder joint has great range of motion, it is not very stable. This makes the shoulder vulnerable to problems if any of its parts aren’t in good working order.

Tendons attach muscles to bones. Muscles move the bones by pulling on the tendons. The upper part of the scapula that makes up the roof of the shoulder is called the acromion. The is also known as the acromion process; this is part of our shoulder blade, or scapula that you can feel sticking up if you rub where the back of your shoulder meets your arm. The acromion process is attached to the scapular spine, and it works with the coracoid process of the scapula to form a solid and stable shoulder joint. The acromion process serves as the point of attachment for the deltoid muscle, which is the major muscle that allows us to lift or abduct our arms. It works with the trapezius to help us shrug.


Shoulder blades lie behind and medially to the shoulders, over the rib cage on each side of the spine; together with the clavicles, they form the shoulder girdle. They make joints with the upper arm bones (humerus) and collar bones (clavicle) but not with the ribs and spine.

Fractures of the scapula occur infrequently, with a fracture of the acromion being an even rarer entity. Acromial fractures constitute 9% of fractures of the scapula, which amounts to 3–5% of shoulder girdle injuries. Fractures of the acromion are generally secondary to trauma, with only a few cases of stress fracture having been reported.
Reports published in English have described stress fractures of the acromion at the base of the acromion extending to the spine of the scapula, neck of the acromion, medial aspect of the acromion, and the base of the acromion only. These cases occurred in young to middle aged patients and were associated with a single violent muscle contraction or repetitive subcritical load to the shoulder.
The shoulder blade (scapula) is a triangular-shaped bone that is protected by a complex system of surrounding muscles. The shoulder blades attach the upper arm and upper back muscles that raise your arms and shoulders and bend your neck backwards or sideways.
Scapula fractures represent less than 1% of all broken bones. High-energy, blunt trauma injuries, such as those experienced in a motorcycle or motor vehicle collision or falling from a significant height, can cause a scapula fracture.
As a result, the mortality rate of individuals with scapular fractures, although not usually direct, has been reported to range from 2% to as high as 14.3%.
Understanding how the different layers of the shoulder are built and connected can help you understand how the shoulder works, how it can be injured, and how challenging recovery can be when the shoulder is injured. The deepest layer of the shoulder includes the bones and the joints. The next layer is made up of the ligaments of the joint capsule. The tendons and the muscles come next.
The shoulder provides maximum mobility and range of motion. Besides big lifting jobs, the shoulder joint is also responsible for getting the hand in the right position for any function. When you realize all the different ways and positions we use our hands every day, it is easy to understand how hard daily life can be when the shoulder isn’t working well.
Scapula Fractures
The scapula or the shoulder blade is a triangle shaped bone which is surrounded by a complicated web of muscles. A fracture of this bone is termed as a Scapula or Broken Shoulder Blade. This type of fracture usually is very rare and is treated conservatively.

shoulder girdle, with the most frequent fractures encountered occurring in the clavicle or proximal humerus. Some sort of functional compensation must occur after malunion, with possible loss of motion, strength, endurance, or reaction time of the shoulder girdle.
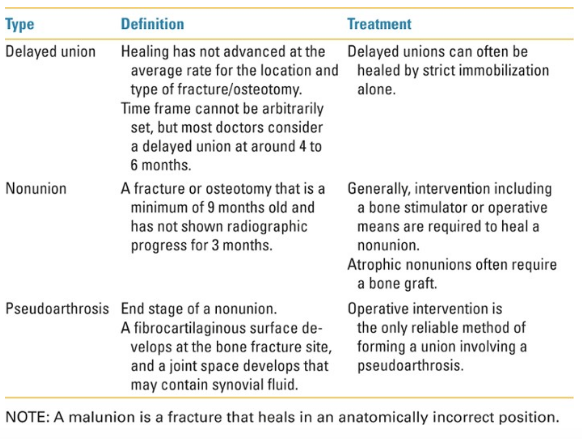
Over the past 2 decades, several studies have documented poor results following nonoperative management of both intra- and extraarticular displaced scapular fractures. Surgical indications for scapular fractures are based on angular deformity and displacement. However, these indications need to be placed in the context of other ipsilateral injuries, as well as patient activity level, hand dominance, and any co-morbidities.
The surgical risks of open reduction internal fixation of scapula fractures have been historically low across many operative series, and it is this relatively low-risk option that should align with the principles of treatment for other fractures. This approach provides the benefit of more immediate pain relief and quicker rehabilitation of the shoulder girdle, with the hopeful prevention of the lasting sequelae of dysfunction more recently discovered in malunions.
Increased surgical experience and surgeon awareness, improved operative approaches, and a higher number of patients who survive high-energy trauma with highly displaced scapular fractures led to good patient outcomes after surgical fixation in properly selected patients.
The presence of a scapula fracture should raise suspicion of associated injuries, because 35% to 98% of scapula fractures occur in the presence of co-morbid injuries including:
- Thoracic/Ipsilateral upper torso injuries (fractured ribs, clavicle/collarbone, sternum) – (80%)
- Pneumothorax (11% to 55% of scapula fractures)
- Pulmonary contusion (11% to 54% of scapula fractures)
- Closed head injuries (42-48%)
- Splenic or liver lacerations 3%–5%.
- Injuries to neurovascular structures (brachial plexus injuries,
vascular avulsions) - Spine injuries (20% lower cervical spine, 76% thoracic spine,
4% lumbar spine)
The reported mortality rate of patients with scapular fractures from the concomitant injuries varies between 2% and 15%.
Acromion Fractures
The acromion process is attached to the scapular spine, and it works with the coracoid process of the scapula to form a solid and stable shoulder joint. Together with the coracoid process it extends laterally over the shoulder joint.

Incidentally, the coracoid is named after the raven, or ‘corvus’, for the unusual beak-like shape of that process. Both the coracoid and the acromion work together, along with the associated muscles of the shoulder, to allow us to shrug our shoulders.
The acromion process serves as the point of attachment for the deltoid muscle, which is the major muscle that allows us to lift or abduct our arms. It works with the trapezius to help us shrug.
Acromion fractures of the scapula are rare and most often occur with concomitant fractures of the ipsilateral glenoid, neck and body of the scapula as sequelae of high-energy injuries. Indications for operative management include symptomatic nonunion, displaced fractures, or acromion fractures associated with other lesions of the superior shoulder suspensory complex.
SUPRASCAPULAR NERVE and SUPRASCAPULAR NERVE PALSY
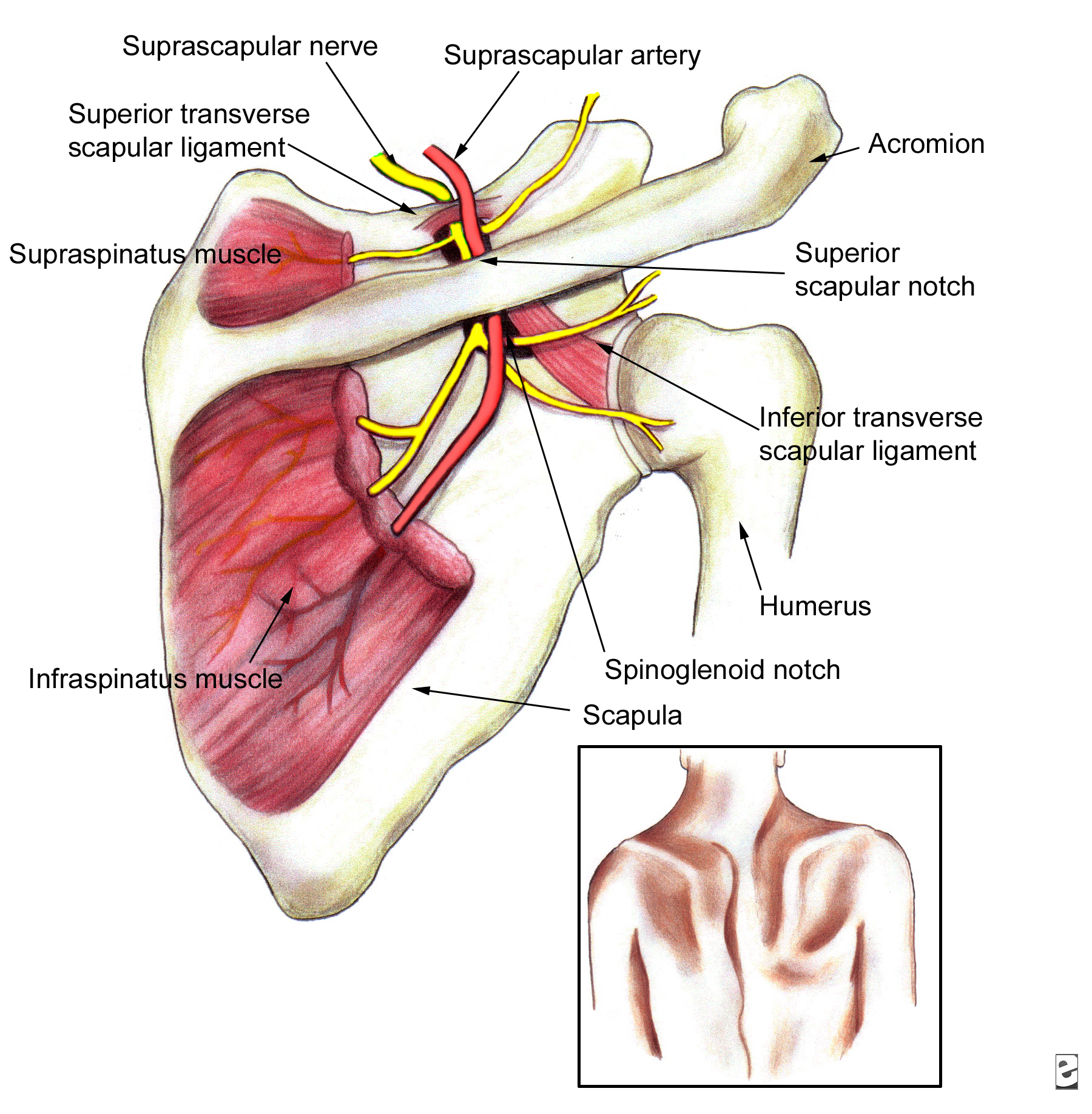
The suprascapular nerve is mostly comprised of nerve roots from C5 & C6. After leaving the brachial plexus, the suprascapular nerve passes under the trapezius and omohyoid muscles Beneath the trapezius and omohyoid muscle, the suprascapular 
nerve enters the supraspinous fossa under the transverse ligament (or suprascapular ligament), courses laterally through the posterior cervical triangle, posterior to the clavicle, then across the superior border of the scapular and into the suprascapular notch. The nerve runs beneath the supraspinatus muscle and curves round the external corner of the spine of the scapula to the infraspinous fossa.
The nerve then continues along the lateral scapula to the spinoglenoid notch, passes under the inferior transverse ligament and enters the infraspinous fossa to innervate the infraspinatus muscle. In the supraspinous fossa, it gives off two branches to the supraspinatus muscle, and in the infraspinous fossa, it gives off two branches to the infraspinatus muscle, besides some filaments to the shoulder joint and scapula.

Its origins are in five nerves coming from five different parts of an area known as the cervical spine (from C5 to T1). The first two nerves (C5 and C6) combine to form what is known as the superior trunk.
The suprascapular nerve along the back of the shoulder can get stretched or compressed enough to cause serious damage. This condition is called suprascapular neuropathy. The result can be shoulder pain and loss of function.
Suprascapular nerve palsy is a relatively uncommon cause of shoulder pain and dysfunction, but can lead to significant disability. It is a fairly rare condition. Most patients present with a progressive dull, burning, and/or aching type pain in the posterolateral shoulder. Pain is frequently worsened with cross-body adduction and internal rotation. Subjective weakness in external rotation and/or abduction may be present. Patients can often recall a specific traumatic event with progressive worsening of symptoms.
When suprascapular neuropathy is suspected, radiography should be performed. In addition to standard views, suprascapular notch and Stryker views can be ordered. Conventional radiography of the cervical spine is warranted if concern exists about a possible radicular etiology for the patient’s symptoms. Shoulder MRI may reveal supraspinatus or infraspinatus muscle edema in acute cases and atrophy with fatty replacement in more chronic cases.
MRI may also reveal a ganglion cyst or other mass such as a paralabral cyst with resultant suprascapular nerve compression. 3T magnetic resonance neurography has been shown to be a valuable diagnostic tool in clinically suspected suprascapular neuropathy. It can demonstrate the nerve abnormality and any secondary muscle denervation changes. Ultrasonography is a reasonable, less expensive initial imaging option. The suprascapular nerve can be identified under ultrasound, and can be used to screen for parascapular ganglia or masses.
EMG is the gold standard and is essential to confirm muscle denervation; however, it is seldom carried out initially because clinical data rarely point to the diagnosis of neuropathy. Only EMG can confirm the diagnosis of suprascapular neuropathy along with a thorough patient history.
REFERENCES:
http://www.mdguidelines.com/fracture-scapula
http://eorthopod.com/shoulder-anatomy/
http://study.com/academy/lesson/acromion-process-definition-types.html
http://www.ivyroses.com/Define/Acromion_Process
https://www.epainassist.com/sports-injuries/shoulder-injuries/scapular-fracture-or-broken-shoulder-blade
http://orthoinfo.aaos.org/topic.cfm?topic=a00359
http://radiopaedia.org/cases/acromial-fracture
https://emedicine.medscape.com/article/92672-workup
Treatment of Complex Scapular Fractures – From the Department of Orthopedics, University of Minnesota, Regions Hospital, Saint Paul, Minnesota ORTHOPEDIC CLINICS OF NORTH AMERICA VOLUME 33. NUMBER 1 JANUARY 2OO2
PDF’s
http://freecontent.lww.com/wp-content/uploads/2014/10/Egol-Ch13-Scapula-Fractures.pdf
http://www.shoulderfractures.info/Data/Scapular-Fractures.pdf
Orthopedic Surgeon Contact:
Peter A. Cole, M.D.
Chief of Orthopaedic Surgery, Regions Hospital
Professor, University of Minnesota
640 Jackson St., St. Paul, Minnesota 55101
Phone: 651-254-3669
Fax: 651-254-1519
Email: Peter.A.Cole@HealthPartners.Com
http://synthes.vo.llnwd.net/o16/US/courses/SYN480/M1712_120113/data/index.html
Thank you for visiting the HOPE TBI Website.
Please take the time to make a comment, share your thoughts, and tell us what impacted you the most and what brought you here:
https://hopetbi.com/reviews-and-testimonials/
Your input is important to the development and growth of this website, and we like to know what is going on out there in your thoughts.
Thank you for visiting us! We look forward to hearing from you.
