Chronic Pain Is No Joke!
So it has been 3 years 5 months and 26 days since the wreck I was in. I just call this 3.5 years to round up when talking with people now.
So much has changed in that 3.5 years….and continues to. The time I have spent adjusting to living with that pain will I believe be lifelong. I have come to believe that pain is a lot like grief, just in a different form. Like grief, there are various stages (also much like grief).
Grief Stages Denial, Anger, Bargaining, Depression, Acceptance
Denial & Isolation with Chronic Pain
The first reaction to learning about trauma is to deny the reality of the situation. “This isn’t happening to me, this can’t be happening to me. I don’t have time for this to happen to me,” – though I think I skipped this first stage initially since I was so out of it. I don’t think I had any ability to conceptualize what I had going on with me…..at least not fully. If I didn’t skip it, I don’t remember experiencing this as a first emotion.
I have always known throughout my life that it is a normal reaction to rationalize overwhelming emotions and to push away dealing with them for most people. This allegedly helps carry us through the first wave of pain or shock. However, when dealing with Chronic Pain that is caused by bodily trauma there is not just one wave or an “initial wave” – there is simply….just…..PAIN.
The reason I said that pain is a lot like grief because pain comes in all forms. Orthopedic, muscular, nervous system related, brain/mental system related, endocrine systems, digestive system, reproductive system, literally every part of the body is engaged in this trauma when dealing with a Polytrauma and Traumatic Brain Injury. Each system can be going through it’s own forms of “grief” or “changes” or they can all be happening at once….overwhelmed…..frozen…..stalled….or shutting down in response to the trauma.
Attempting to take all that in and learning that no one around you really truly understands is incredibly isolating. Being unable to put to words how you are feeling when you have never been put into a place in your own life to need words to describe such a horrific continual experience feels isolating. I would deny deny deny that this was actually happening – yet the pain made that reality absolutely undeniable. All I could think of was PAIN….where the hell is all this pain coming from? There was so much I couldn’t pinpoint a starting place. It was like someone wrapped me in a warm pain blanket that was turned up to the highest level possible without relenting for months and months (literally)
Anger with Chronic Pain
As the effects of denial and isolation change in their dynamic, reality and its pain re-emerge stronger than ever. I admit I was not prepared for this emotion which continually hits me in random waves. The anger may be aimed at inanimate objects, our healthcare providers, complete strangers, friends or family. Anger may be directed at the person we perceive that hurt us or even angry at ourselves. Often times feeling guilty accompanies being angry and for some people, this makes them angrier. Sometimes being angry is a side affect of the trauma….especially if dealing with a head injury and the emotional center of the brain has been damaged.
As anger relates to chronic pain though – at least for me, the anger comes from not being able to do what I used to do. Anger at having this affect my life, my mobility, my independence in caring for my own body, and change my normalcy to something I no longer recognized. Anger at literally feeling like a prisoner in my own body and having expectations that are not realistic for the healing required for the injuries themselves, or my ability to deal with the injuries. Anger about missed injuries, or those that are not healing as planned. Angry at feeling dismissed, not taken seriously by anyone outside of ourselves when I say I am hurting. Angry about being financially destitute and unable to provide for my family the way I used to. Angry that I am hurting at all.
Some things that come with chronic pain and anger
- Sudden muscle spasms or pain “flares”
- Inability to take a deep breath or feel like the room is collapsing/shrinking around you
- Feeling okay and then a wave of anger appears from nowhere and leaves just as suddenly as it came
- Low tolerance for things you were able to tolerate before (everything seems exaggerated when angry or hurting and angry)
- Guilt or shame for angry outbursts (when pain unrelentless or spiking) after you have had time to calm down and think about it
- Appropriately angry about something but then transferring that anger to someone else about something completely unrelated to what you are really angry about
Bargaining with Chronic Pain
The normal reaction to feelings of helplessness and vulnerability is often a need to regain control. Let’s face it, with a polytrauma where you cannot walk/have difficulty walking, where you have to have someone feed you, dress you, wipe your butt for you, bathe you and leaves you feeling completely helpless – is a complete loss of control in its most humbling form
Admittedly I have always had a leadership/controlling personality. I enjoy doing a job well and got value from how others viewed my ability to lead, accomplish, and successfully complete something. I loved my independence and enjoyed working and breaking new ground in almost every aspect of my life. Now I am trying to reinvent me.
Then BAM – chronic pain comes in and strips down any ability to control…at least completely what’s going on in your own environment – your own body. This is truly where things spiral a bit…I personally tend to get consumed with dark thoughts and overthinking my care or lack thereof. I think about how I can negotiate better treatments, better documentation, a better more proactive diagnosis. It becomes almost obsessive. I have to admit that there is a fine line between bargaining and advocacy for oneself (which has actually served me well orthopedically). However, along with bargaining comes some pretty repetitive self-talk. This can be a strength and a weakness in the recovery process.
- If only they had researched my injuries and found solutions sooner my rehab would have been shorter
- If only they did the basic tests they would have caught that faster
- If only I got a second opinion from another specialist
- If only I tried to push myself more
- If only I didn’t push myself so far
- If and if and if and if…even with God/Universe “God if you help me get through this pain I won’t do this”…..or “I will do this” just to help me deal with this pain that is controlling my life and every breath
- Getting lost in “what if’s” and “if only’s” consume every decision in this stage. This can lead you in directions of improved care, or hamper your progress – there is a fine line for sure
- The desire to have my life return to the way that it used to be, restored to no pain zone, the ability to do more without pain, the desire to cope with the pain
- The desire to go back and keep wreck from happening altogether
Depression and Chronic Pain
There are many types of depression out there. There are 2 types of depression when dealing with grief and loss that appear most often though. The first one is a reaction to relating to the loss. Sadness and regret predominate this type of depression. We worry that, in our grief, we have spent less time with others that depend on us. This phase may be eased by simple clarification and reassurance. We may need a bit of helpful cooperation and a few kind words.
The second type of depression is subtle and, in a sense, perhaps more private. It is our quiet preparation to separate and to bid our old self as we knew it farewell, while dealing with our “new normal” and the chronic pain that we now live with.
With a polytrauma or traumatic brain injury a person is often on a lot of medications to control various injuries or mood disorders. Some of these medications can actually cause depression. It is hard sometimes to tell where the depression is coming from and requires a thorough awareness of the patient’s medical history. When dealing with depression in myself I learned my depression was there due to many factors – all secondary to the wreck and the ripple affect of all the injuries. I got news for ya’ – peeing yourself in public because you aren’t able to get to the bathroom fast enough when that urge hits ya, living with a chronic headache pattern, chronic pain, and short term memory loss can be very depressing in and of themselves – and that’s just the basic stuff. Now add money problems because you cannot work, being unable to pay bills on time, and all the other normal life stressors which now seem bigger than the pain some days and that depression can drag you down like a cinder block tied on your back while you are in life’s swirling pool.
Seeing your friends lives go on, seeing your family move on while you seem stuck in the same vicious circle – wake up pain, walk – pain, exercise – pain, carving your way through the day until you can go to sleep to hopefully escape pain – (some days that actually works…… over time….until a pain flare)
When depression hits me hard, I notice that grief that holds hands with depression has a bit of a tighter grip. Sometimes this stage feels as though it will last forever and can feel truly overwhelming. I also notice that depression is harder to control when hurting. So being in chronic pain is often not necessarily related to a mental illness (though can be related to endocrine and hormonal imbalances caused by trauma as well), but rather a response to hurting so much for so long and feeling frustration over adjusting to that “new normal”. I also have realized that my pain tolerance has changed dramatically over the last 3.5 years. I can withstand a lot more pain that I used to on some levels – not so much on other levels. I also notice my depression has changed with that adjustment.
Also, by golly, depression is an appropriate emotion when experiencing great loss. A lot of people….professionals even – act like it is some kind of an unnatural process. That cloud of intense sadness that consumes one’s being when they feel like they are all alone in their experiences and realize that their life will forever be dramatically different is a real sense of loss. I really have to guard myself against that whole feeling of “what’s the point in living” “why did I survive” “what am I here to accomplish” and force myself to focus on positive self-talk.
Depression is not a “state to be fixed”, something to “snap out of”. Though I do believe it is important to recognize that our feelings are very real, but do not always tell us the truth about the situation. Grief is part of the healing process. Chronic pain is part of my life now. Some days I manage it better than others – some days….not at all. If grief is a process of healing, then obviously depression is just another important step on that journey. Allowing myself to experience it (yet not get stuck in it) is also an important part of that process.
Depression is also not consistent and can last a few moments to never ending cycle from day to day. It’s okay to cry here and there for 5-15 minutes at a time my counselor told me. That is healthy. It’s a problem though to be really addressed if it consumes your life so much you can do nothing else because of feeling so depressed. If all I can do is think of the depression and cannot quit crying and am withdrawing so much that I am neglecting myself (eating, hygiene, activity participation), then more professional help may be needed.
Acceptance and Chronic Pain
Not everyone is able to reach this stage. I still struggle with this stage myself on a daily basis in my rehabilitation process. My counselor calls my ability to accept the changes to my life, my body, my new normals as a need to have “radical acceptance”. Let’s face it….something radical has happened to me and therefore requires a radical form of acceptance.
Sometimes seeing beyond our anger or denial makes this more of a difficult process. This phase is marked by being calm. This is not necessarily a period of happiness and it is imperative to distinguish this from the apathy or withdrawal that I spoke about in depression.
So what does it mean anyway to have a radical form of acceptance?
Radical Acceptance to me, means completely and totally accepting something from the depths of my soul and with mind and whole beingness. I have to face the reality that I may never be able to work in the same way that I used to. I have to accept that I am at my medical best in some things, still improving in others, and that yet others may never improve (or may even get worse). It means accepting I may need to use a cane, go to counseling, change the way I do things. It means accepting that chronic pain is just a part of my life now and learning to work around it as best I can. It means knowing that my nerve damage may never heal (or it might) and accepting that. It means to stop fighting reality.
Radical acceptance means that I do not allow myself to feel that rageful anger in my stomach when I am unable to do something I used to be able to do. It means not seething with resentment or bitterness when I see others who have similar injuries doing more than I am capable of with my own body. Radical acceptance means, learning as much as I can, teaching others to do the same, and moving forward with my life.
Radical acceptance is way easier to talk about and understand than it is to actually put into practice in every moment of every day. There are a ton of obstacles that come up to challenge accepting where I am at now. I do know that if I stop fighting all of this, eventually I will suffer less.
What Radical Acceptance is not: It is not giving up. It is not tolerating being mistreated or accepting a misdiagnosis. It is not stopping the ability to advocate for oneself or others. It is not just accepting diagnoses as they are without researching the options thoroughly. It is not giving up on caring about or speaking up for myself or others. It is not about being as silent as a church mouse in a corner with no thoughts and ideas of my own. It is not about even….. being Radical (which some interpret as crazy, out of control, explosive, or some other such adjective).
Summary:
Coping with a polytrauma, traumatic brain injury, any type of grief, and loss really…. is ultimately a deeply personal and singular experience — nobody can know EXACTLY what you are going through.
There are many stages we all go through in our recovery process. These stages closely resemble the stages of grief. There is no set time frame assigned to experiencing each stage, or a particular order in which we experience these stages. Sometimes a person may never get to the Acceptance stage. This is however, the goal for myself.
Acceptance is often misinterpreted by others as the person being “all right” or “okay” with what has happened to them. This is not the case. Some people reach acceptance right away. Most people though don’t ever feel okay for years, if ever. By achieving a level of “acceptance” a person is choosing to learn to live with their new normal self and move forward with their life.
It is not uncommon to repeat the various stages or be focused on one particular stage. Chronic pain can directly affect the way a person processes these stages as well.
(Over recent decades, a reasonable amount of data has been generated which suggests that greater acceptance of chronic pain is associated with fewer pain-related difficulties, such as distress and disability, and better overall quality of life (for reviews, see: McCracken & Vowles, 2014; Scott & McCracken, 2015; Vowles & Thompson, 2011). http://www.bodyinmind.org/pain-acceptance/
About the 5 stages of grief:
In 1969, Elisabeth Kubler-Ross introduced the stages of dying in her book, On Death and Dying.
Before her own death, Elisabeth Kubler-Ross and her co-author, grief expert David Kessler adapted her well-loved stages for grief in their book, On Grief and Grieving.












 In the beginning I was at the point when I couldn’t easily reset myself, so I would say “BRAIN TIME”, go in my room (or they would have to leave my room), and I would stay there until things settled down in my head. No interruptions, no calls, no questions, door shut. Sometimes this was moments, sometimes minutes, often hours, or occasionally days. I needed absolute silence, a dark room, a warm heavy blanket and to lay down perfectly still. I slept a TON.
In the beginning I was at the point when I couldn’t easily reset myself, so I would say “BRAIN TIME”, go in my room (or they would have to leave my room), and I would stay there until things settled down in my head. No interruptions, no calls, no questions, door shut. Sometimes this was moments, sometimes minutes, often hours, or occasionally days. I needed absolute silence, a dark room, a warm heavy blanket and to lay down perfectly still. I slept a TON. Two and a half years after the trauma I started to return to driving. I would learn my inner compass was missing/broken. I was horrified to find myself LOST after taking my kids to school. In fact, I couldn’t remember how to get there….a trip I had made hundreds of times before. I used a GPS because it was like I had never been there before. Now THAT made me feel coo-koo….I didn’t understand. Then I got lost heading home. I literally ended up 20 minutes in the opposite direction because I couldn’t remember what to do or how to get where I needed. GPS became an absolute crutch. As time has gone on, I have gotten better about figuring out my routes. Often times I could think of where I needed to go…yet applying it to real life outside my head was a different reality entirely.
Two and a half years after the trauma I started to return to driving. I would learn my inner compass was missing/broken. I was horrified to find myself LOST after taking my kids to school. In fact, I couldn’t remember how to get there….a trip I had made hundreds of times before. I used a GPS because it was like I had never been there before. Now THAT made me feel coo-koo….I didn’t understand. Then I got lost heading home. I literally ended up 20 minutes in the opposite direction because I couldn’t remember what to do or how to get where I needed. GPS became an absolute crutch. As time has gone on, I have gotten better about figuring out my routes. Often times I could think of where I needed to go…yet applying it to real life outside my head was a different reality entirely. If they turned their backs to me I would ask them to turn around and repeat what they said. Some folks are super accommodating, some act put out by this. Often times folks think you aren’t interested in listening or you do not care about what they said. It wasn’t that, I just couldn’t process what they were saying. Sometimes the words didn’t make sense. It’s like I was listening to a foreign language sometimes. Sometimes it was like I could see their mouth moving, hear noise coming out, yet couldn’t make out the words. This was maddening. Oh! if I was doing something and all my focus was on it (like typing or reading), forget about me hearing you..it just didn’t happen.
If they turned their backs to me I would ask them to turn around and repeat what they said. Some folks are super accommodating, some act put out by this. Often times folks think you aren’t interested in listening or you do not care about what they said. It wasn’t that, I just couldn’t process what they were saying. Sometimes the words didn’t make sense. It’s like I was listening to a foreign language sometimes. Sometimes it was like I could see their mouth moving, hear noise coming out, yet couldn’t make out the words. This was maddening. Oh! if I was doing something and all my focus was on it (like typing or reading), forget about me hearing you..it just didn’t happen. After the polytrauma I seemed to lose the ability to feel hunger or fullness. For some bizarre and I am sure possibly scientific reason I lost my appetite or desire for food in general. No more interests, no more favorites, no more “cravings”, and no more enjoying the things I used to enjoy before. My sense of taste and smell had changed. Some of the things I enjoyed before now repulsed me. Smelling certain types of food cooking was enough to turn me “green” (sick). Just looking at certain types of food was repulsive. The connection with food emotionally seemed to go on vacation. In fact, if I wasn’t brought my meals in those early months and sometimes still…I just wouldn’t eat because I would just forget to eat or have no interest in it.
After the polytrauma I seemed to lose the ability to feel hunger or fullness. For some bizarre and I am sure possibly scientific reason I lost my appetite or desire for food in general. No more interests, no more favorites, no more “cravings”, and no more enjoying the things I used to enjoy before. My sense of taste and smell had changed. Some of the things I enjoyed before now repulsed me. Smelling certain types of food cooking was enough to turn me “green” (sick). Just looking at certain types of food was repulsive. The connection with food emotionally seemed to go on vacation. In fact, if I wasn’t brought my meals in those early months and sometimes still…I just wouldn’t eat because I would just forget to eat or have no interest in it. I have come to realize that my thyroid-pituitary-hypothalmus axis was way off. My hormones were all over the place and apparently I rattled that temperature control center of my brain pretty good.
I have come to realize that my thyroid-pituitary-hypothalmus axis was way off. My hormones were all over the place and apparently I rattled that temperature control center of my brain pretty good.
 sporting events, and Pep Rally’s are an amazing memory. As I grew into an older adult some of my music interests changed, yet I still held on to that love of music (which my parents would have probably argued on some days was noise to them). When I worked in Emergency Medicine, I love the sound of the sirens, the pager going off, the squelch on the CB or radios, the multiple directions and decisions that had to be made to save a life. I knew by their sounds whether it was “go time” or not.
sporting events, and Pep Rally’s are an amazing memory. As I grew into an older adult some of my music interests changed, yet I still held on to that love of music (which my parents would have probably argued on some days was noise to them). When I worked in Emergency Medicine, I love the sound of the sirens, the pager going off, the squelch on the CB or radios, the multiple directions and decisions that had to be made to save a life. I knew by their sounds whether it was “go time” or not.

 people’s lips to understand what they were saying. Sometimes still I will see lips moving, know they are talking, yet understand NOTHING. I have learned to ask for repetition a lot. Sometimes I just act like I know what they said….nod….and smile. I learned little tricks, like wearing earplugs, sunglasses, carrying a blanket to cover my head with, lots of those types of things to cocoon myself from the auditory assaults of whatever environment I was in.
people’s lips to understand what they were saying. Sometimes still I will see lips moving, know they are talking, yet understand NOTHING. I have learned to ask for repetition a lot. Sometimes I just act like I know what they said….nod….and smile. I learned little tricks, like wearing earplugs, sunglasses, carrying a blanket to cover my head with, lots of those types of things to cocoon myself from the auditory assaults of whatever environment I was in. 
 A ripple effect that swirls and snatches and seeks to destroy not just the patient, but the family, the spouse, and friendships of that patient as well.
A ripple effect that swirls and snatches and seeks to destroy not just the patient, but the family, the spouse, and friendships of that patient as well. Any delayed treatments, or misdiagnoses, or haggling over care of the patient (whether by the family or the patient themselves) causes additional added stressors, which impacts the ability to heal in a timely fashion.
Any delayed treatments, or misdiagnoses, or haggling over care of the patient (whether by the family or the patient themselves) causes additional added stressors, which impacts the ability to heal in a timely fashion.
 The financial stress will compound quickly. The person injured, if a working parent, may be unable to return to work for a period of time…if ever. This creates a massive financial dynamic shift for the whole family. If insurance is not available, or does not cover all of the medical bill this can spell financial ruin for a family. Not many individuals or families are in a financial position to endure a catastrophic injury/event. This is only compounded when the parent that is left working loses their employment because they are taking too much time off work to care for their spouse/family member. This can exponentially compound the stressors in the household.
The financial stress will compound quickly. The person injured, if a working parent, may be unable to return to work for a period of time…if ever. This creates a massive financial dynamic shift for the whole family. If insurance is not available, or does not cover all of the medical bill this can spell financial ruin for a family. Not many individuals or families are in a financial position to endure a catastrophic injury/event. This is only compounded when the parent that is left working loses their employment because they are taking too much time off work to care for their spouse/family member. This can exponentially compound the stressors in the household.












 brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.
brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.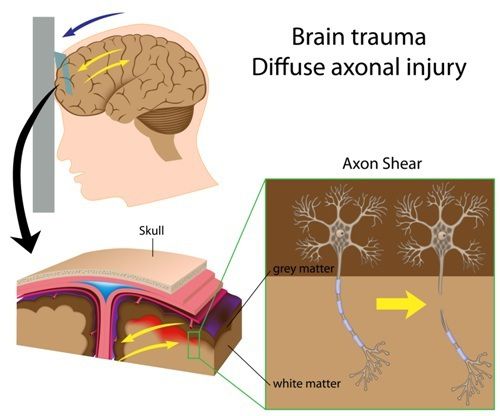 PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage.
PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage. Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.
Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.

 not own it as my own, but rather something I experienced.
not own it as my own, but rather something I experienced. may be thinking wow thanks for sharing information I didn’t need to know. Why does this matter to me as a reader? Good question!!!
may be thinking wow thanks for sharing information I didn’t need to know. Why does this matter to me as a reader? Good question!!!


 I have been thinking about what to write today, January 4, 2017 for about a month now. Here I sit trying to think of how to form the words that swim in my mind and express them in a way that makes sense to anyone else but me.
I have been thinking about what to write today, January 4, 2017 for about a month now. Here I sit trying to think of how to form the words that swim in my mind and express them in a way that makes sense to anyone else but me.
