What Exactly is “Standard of Care” as it relates to the medical community?
The “medical standard of care” is typically defined as the level and type of care that a reasonably competent and skilled health care professional, with a similar background and in the same medical community, would have provided under the circumstances that led to the alleged malpractice.
A diagnostic and treatment process that a clinician should follow for a certain type of patient, illness, or clinical circumstance.
The level at which the average, prudent provider in a given community would practice. It is how similarly qualified practitioners would have managed the patient’s care under the same or similar circumstances.
**********************************************************************
I have learned over my entire life through various experiences; also being in the medical field for most of my adult life as a healthcare provider in some way, shape, or form that the Standard of Care is as varied as each personality that goes along with the person representing that Standard of Care.
When I had patients I always tried to give them the best of me and my knowledge of my acquired training at that time. When I came across something I didn’t know (which was a continual learning process for sure)…. I immersed myself in learning about the things I didn’t know how to answer for what I was specializing in at that time. That was my way of making sure that I didn’t have that same issue come up again. I guess I just assumed (yes, we know the misnomer of what assume means) that this is how all people sought to learn when they had a passion for medicine. Specialists in a field even moreso…beyond the norm even.
Specialists, surgeons, Department heads I guess I always expected more of those folks. Surely they kept up on all the latest trends, the newest studies, the symptomology associated with the topic(s) they specialized in. Surely they could spot a problem, would assure that the best outcome for the patient was acquired, especially in favor of positive outcomes with their name attached to it.
Surely I could look at them, listen to them use my voice to communicate with them, and trust they knew what they were talking about because after all, their fervor and thirst for knowledge was above and beyond what the average medical professional entailed. Certainly more than what I was trained to know.
So it only made sense that on that fateful day when I became the voiceless patient, clothing cut off to stark nakedness in an emergency room with massive injuries, multiple broken bones, head injury, and clinging to life with each labored breath…..that the sheer mechanism of injury (severe car wreck with ejection and other driver pinned and needing to be cut out) should have demanded a certain Standard of Care from every provider I came into contact with, within that first year, and every day after that.
I have had some really great providers. I still have some great providers. I want to say that first. There are a handful who have done their due diligence and even exceeded the Standard of Care. They are the ones that listened. That actually enjoyed their job and their patients. They are also the ones that keep up on the current and updated things in medicine, ironically enough. They are the ones who think of ways to make things happen instead of making excuses of why they cannot make things happen. They are the providers that never give up on you and take risks to better your quality of life. They are few but mighty. These are the providers I have learned a lot from and have enormous respect for.
The providers who fell short on their Standard of Care, or didn’t even attempt to live up to it….. Those providers left me impacted in ways that created a ripple affect that delayed my care, caused me further injuries, and exacerbated things for my recovery process….and not in a positive way. They are the providers who didn’t listen. Who jumped to conclusions based on opinion rather than facts. They fed off of other reports by other providers that also did not care, did not document properly, or dropped the ball in some fantastic and important way; perhaps even adding wording that invalidated the injuries that actually were quite legitimate and yet ignored. These are the providers that I felt I knew more about my care and the latest treatments available than they did (yes even if they touted themselves as specialists in that field). These are the providers I lost respect for, or never had the chance to establish such for.
The Standard of Care cannot be overstated in its importance. If you specialize in a field, learn all you can about that field. Study it, know it, and be willing to learn more about it. Medicine is changing daily and if a patient brings you the current studies, be grateful. If they discuss them with you and you have never heard about them, go look them up and research them yourself. Knowledge can only make you better at your craft. If you cannot listen…truly listen to your patient when they say they are still suffering – you are in the wrong line of work. Go on a quest, do no harm, and advocate for your patients.
The Standard of Care echoes through many professions, yet in this particular post we just address the medical view as a patient, medical advocate, a Survivor.




 brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.
brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.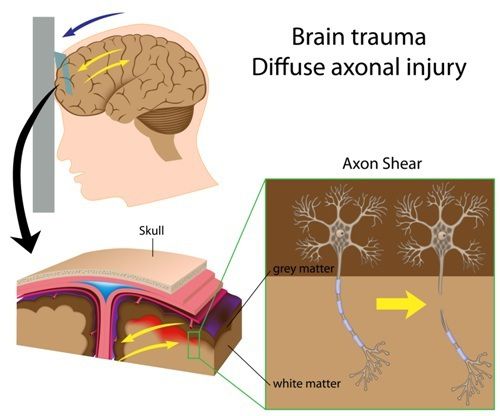 PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage.
PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage. Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.
Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.