A Personal Update: Honoring My Voice, My Values, and My Path Forward
Many of you know that for the last 6 years, I have had the blessing of co-hosting a brain injury radio show monthly (and sometimes twice a month) with Kim Justus on “Recovery Now” through Blog Talk Radio. It has been one of the most meaningful parts of my rehabilitation journey.
What began as a platform for education became something much deeper, a space for healing, connection, advocacy, and purpose. It also became an important part of my identity, both personally and professionally. When the platform we were using suddenly closed down without adequate warning, we were forced into a 9-month hiatus while we navigated our own personal events in our lives. In the meantime, we were also exploring various options and platforms where we could settle in, to continue hosting the brain injury radio show at its new hosting site. We finally were able to plug back in and were thrilled to offer our show not just once a month, but twice per month, and things were developing nicely.
As someone living with and navigating the realities of brain injury and polytrauma, this work has never been just “content.” It has been a lived experience, growth, and a way to support others walking similar paths.
Because of that, I want to share something openly and honestly with my followers, those who have approached me with questions, and those who are supportive in the Health and Wellness Communities:
I am no longer part of that particular radio show.
This was not a decision I made or agreed with, and it was not one I initiated.
A Clarification That Matters
There may be messaging that suggests I chose to step away to pursue other goals. While I am always growing and expanding in my work, my departure from the show was not a personal decision to leave.This transition followed a difference in perspectives that extended beyond the scope of our work together.
I share this not to create division, but to provide clarity with honesty and respect.
Where I Stand Personally and Professionally
I have taken a while and personally debated whether to address any of this publicly. However, so many of you that have been loyal over the years through your messages, support, and as a part of our listening audience have been reaching out because you noticed there were some changes. I felt I owed you some clarifying commentary.
Many of you know that I keep my professional platforms intentionally nonpartisan and focused on education, healing, and empowerment as much as possible. After all, Brain Injury, Polytrauma, and the need for support does not discriminate based on personal beliefs or personal values.
At the same time, I am also a human being with my own personal values, and don’t often shy away from speaking my mind….especially in my personal circles.
On one of my personal social media platforms, I have spoken about issues related to:
human rights
civil rights
advocacy
dignity and ethical treatment for all people
These are not positions I take lightly. They are rooted in my lived experiences, my work in advocacy, and my belief that all people deserve to be treated with respect and humanity as part of the human race.
I understand that not everyone will agree with my personal views, might find them offensive, and that’s okay.
But I want to be clear:
I will not apologize for standing in alignment with my values when it comes to human dignity, advocacy, and the protection of others.
That is not political to me.
That is foundational to who I am – both as a person and as a professional.
Advocacy Is Not Selective
In my work, I support individuals navigating complex medical systems, trauma, and life-altering conditions.
Advocacy cannot be conditional. It cannot depend on convenience, comfort, or agreement. It often boldly goes where others avoid or are unsure how to represent what needs to be said.
Whether someone is a patient, a provider, a caregiver, or part of any system…..accountability, courage, and compassion must coexist.
Continued Support for the Broader Mission
I want to be clear that my release from the show does not change my respect for the work being done by the show, the network, or within the broader brain injury community.
I continue to support the mission of education, advocacy, and awareness that platforms like HOPE TBI, Recovery Now, Brain Injury Radio, the TBI Network, and other like-minded folks aim to provide.
My commitment to this space remains strong, and I will continue contributing through my own platforms, including HOPE TBI and my other ventures.
Moving Forward
While this transition was not one I specifically chose, it has created space for me to continue expanding my work in ways that remain fully aligned with my mission.
Through HOPE TBI and my ongoing advocacy, I will continue providing education, awareness, and support to those navigating brain injury and recovery. In fact, look for some upcoming surprises and growth opportunities in 2026 involving HOPE TBI and the path forward.
This work has always been, and will continue to be, about helping others find clarity, strength, and hope. It will always remain an extension of my love for the global community.
To Those Who Have Supported Me
To those who have listened, learned, shared, and grown alongside me over the years – thank you. I am truly blessed to have your support.
Your trust, your stories, and your resilience have meant more than I can fully express. I look forward to many more years of hearing from you and sharing with you.
This is not the end of my light or my voice. I can assure you of that. It is simply a shift in where and how that voice continues, and where that light continues to shine.
Please take the time to make a comment, share your thoughts, and tell us what impacted you the most and what brought you here: REVIEWS and TESTIMONIALS
Your input is important to the development and growth of this website, and we like to know what is going on out there in your thoughts.
Thank you for visiting us! We look forward to hearing from you.
With a heavy heart we share our loss, wish a peaceful transition and reflective thoughts to our
dearly departed HOPEster…..Jesse Jhon Andrews.
Jesse Jhon Andrews lived a life that was complex, creative, and unforgettable. His story is not easily summarized, because he was not a man of simple lines. Jesse felt deeply, created passionately, and saw the world through a lens uniquely his own. His music, writings, and the lasting imprint he left on those who knew him continue to speak even in his absence.
We invite you to visit Jesse’s Memory Page, where his life, his work, and the stories shared by those who loved him are preserved. This page honors not just his struggles, but the incredible brilliance, depth, and one-of-a-kind spirit that defined him. This page serves as a place where his story can continue, where his voice can still be heard through the work he left behind, and where those who knew him, or wish they had, can connect with the legacy of a life that was lived fiercely and uniquely.
Explore Jesse’s Memory Page by clicking the word below that says “HERE”:
Today marks a milestone in the life of myself and my family. Today is the 11th-year survivor-versary of the wreck that, in part, changed the course of all of our lives.
While it remains factual that it was myself and our youngest son involved in the actual wreck itself all those years ago, the family as a whole would become and remain affected as a result of its aftermath – for years to come. The rehabilitation journey has not been for the faint of heart and continues…albeit in different ways now than when it all began.
There have been many things involved that have gotten me to this point in my life – which I guess I would call the “survivors plateau”. Many things that cause me to reflect a bit deeper each year at this time.
On the positive (effective) side, I could speak about the great care of many healthcare professionals; the unwavering support, love, struggles, and sacrifice of time and energy of my family; how clinging on to HOPE, my deep-seated faith, and a healthy dose of daily gratitude has helped us traverse this seemingly insurmountable experience. I could speak to many details, many therapies, many opportunities for growth, successes, and immense blessings that have come into our lives….with and without concentrated and unbridled effort and determination.
On the negative (noneffective) side, I could speak about the chronic physical and emotional pain that still riddles my body and our lives in various ways; I could speak of the continual setbacks and disappointment…and the deep and very personal losses that no one ever sees – that continue to wreak havoc at many levels – levels that force me into a daily field of emotional landmines that seek to obliterate all that I continue to accomplish and overcome. I could speak of the financial toll it has taken and continues to take from our family and my body;
However, what I want to focus on in this writing is not far from either of these things, but a valuable idiom that has been the consistent and steady foundation of all of these things over time.
What I want to write about today, is a lesson that we could all come to appreciate and give an open arms welcome to…..and that is the gift of the things that happen, come to us, appear, or work out at the last minute, sometimes in ways we never saw coming, sometimes as a result of seriously difficult and seemingly hopeless moments – a glimmer of light, a breath of air, right when we need it and often in unexpected ways. I want to write about the good dose of courage required to face a world without this relief, and the sheer awe created as it rises up to present us with a much-needed outcome in the 11th hour of our stripped-out moments.
Some may be wondering what I mean when I reference this verbiage “the 11th hour”. Let me take a moment to reflect on some various views of this, and how it can be used in various contexts…….
The phrase “at the 11th hour” is an idiomatic expression (cannot be understood according to its literal meaning) or allusion (subtle way to mention something familiar) that means at the last possible moment or just before a deadline. It suggests that something is happening or being done in the final moments before a crucial event or situation. (3). In a broader sense, “at the 11th hour” can refer to any situation where action or intervention takes place when time is running out or when it seems almost too late to achieve a desired outcome. It implies a sense of urgency and often conveys the idea that there was little time to spare or that the situation was in a critical state before the last-minute action was taken.(4)
The 11th hour means the latest possible time before it is too late. It is a phrase that means “at the last moment”. It is taken from the Bible passage in Matthew 20 verses 1 – 16 where Jesus taught the Parable of Workers in the Vineyard. The eleventh hour miracle is a miracle you get when it looks like time is running out on you. (1)
Perhaps the most celebrated “eleventh hour” was 11 a.m. on November 11, 1918, the “eleventh hour of the eleventh day of the eleventh month” — “Armistice Day,” which brought an end to World War I.(2)
Note that the Roman time system referred to twelve ‘hours’ from sunrise to sunset (and twelve hours of the night from sunset to sunrise). So the eleventh hour was by definition the period just before the end (of the day). ~Tim Symington (ironically posted in 2014 – 11 years ago)
Ultimately, the phrase “in the 11th hour” has multiple spiritual meanings as well. Being a person who clings to their personal faith as a way-shower…I share these things as specific examples:
Refusing to give up – this supports that idea of not giving up too soon, not giving up the effort, or the attempt, even if things are going, or appear to be going, badly. This is often the time when everything points to needing to give up, and then a solution or miracle comes.
God’s Timing – the idea that God will intervene at the last minute, even when things seem hopeless.
Claim Opportunities – this relies on the actual effort and choice to take the opportunities, or use the resources given to us
Delayed Blessings – this is reflected by the ripple affect of blessings coming to us in various forms long after the time we would have experienced them in a traditional time continuum.
Today, as I write this. I am reminded of how, in the 11th hours of many days…. I have been lifted and plucked from the bowels of depression, exhaustion, and at times a concentrated form of aloofness, or lack of desire to go on.
As I write this, I am honored to share my progress with all of you as a testament of the fruition and reward of hard work, resilience, and sheer grit. I have been managing and expanding on the services I provide in my business; am in school still and working towards a Higher Education Degree to represent my new life. I am making great strides to return to a modicum level of activity and vocational satisfaction in the form of a successful reckoning and comeback tour. I continue each day to show up for my life. I volunteer, advocate, and continue to give back as I am able. Life is hard. Life is a bitch. Life is tough……but my goodness is it also rewarding.
Here I am in all my unique complexities in this 11th year of my rehab journey and literal reinvention of my life.
Today is not without its challenges, failures, learned mistakes, or hard lessons that this process continues to shed light on. Today though, in the 11th hour of this Anniversary, I also celebrate a life I have grown to be proud of. A life shed of toxic people from my inner circle. A life that keeps giving me unexpected and sometimes delayed blessings. A life that keeps giving me miracles with each breath I have been allowed to experience each and every day. A life that has given me a life partner/husband/friend who inspires, supports, and loves me with selfless representation. A life that continues to allow me to witness the love through others (specifically those close to me, but through humanity in its finest glory too). A life that injects an ever-present presence of deep dramatic chasms and last-minute solutions that continue to shape the tapestry in the valleys of my world.
Today I face a turning point, a choice; an opportunity in the 11th hour of this day….. to define my next steps and wear my confidence like a cloak of joy, exalted, as I pay it forward to the next generation.
It takes a healthy dose of humor and unyielding humility to reach the 11th hour. A place when all may, at times, seem lost; when the precipice, or teetering of survival and destruction (or light vs darkness), vie for the same spotlight and seeks to own the moment – whatever that moment may be.
It takes determination to reach the 11th hour. A place that lays naked…. and bares all the beliefs, values, and character of the individual thrust into its path.
It takes realization to TRUST in the 11th hour; to trust that life goes on and will continue to evolve with or without our decree, consent, or approval.
The 11th hour carries the rescuing we all need at times and then sheds the stress, strife and hopelessness from our midst repeatedly; a place where all things come full circle.
Check out our latest page addition to our Site. HOPE TBI has partnered with Vital Ability, LLC to offer our readers access to another resource:
The “Brain Injury Mentor Program” puts you in contact with a mentor who connects with you on a one-to-one basis, helps inspire you, and helps you figure out how to overcome roadblocks. They provide you with resources and tools based on their own experiences, connections, and self-advocacy strategies.
They are someone that is knowledgeable about the medical field that can listen, relate, and be supportive, through a research and strengths-based approach, as you navigate your own brain injury process.
Human beings are creatures of time. We are preoccupied with what time it is, getting somewhere on time, keeping calendars, planners, setting timers, setting alarms, and wondering how much time is left so we can stretch our budget until our next payday, and even how much time is left in our current life. Maybe we are even too obsessed at varying moments throughout our life and as a society as a whole.
Some, like Albert Einstein would even say that time is an illusion…a distraction to keep us shackled between the past and the present. To many physicists, like Carlo Rovelli, who says “…our perceived reality is a sequence of events (past, present, and future), and we assign the concept of time to that sequence” – thus making time an illusion.
Other physicists would say that while we experience time as psychologically real, time is not fundamentally real.
The sensation of time seeming to perpetually “freeze” often arises as a byproduct of awe or amazement, that rare but overwhelming feeling of reverence we experience when witnessing something wonderful or miraculous.
Interestingly, one of the strangest side-effects of intense dread or fear, is the magnification and simultaneous slowing down of time. This is often put into visual form in movies when we see a specific moment or scene slowed to a very dramatic and obvious pace that seems surreal.
Additionally, a lot of us find ourselves losing track of time. Among all the things that can cause this losing track of time phenomena, there are some medical things to consider as possibilities. For example, how fast we are able to process our sensory input along with what we experience with our senses can change our perception of time. There are even a few studies that show that an auditory event can appear to last longer than one that we see visually. According to one study, we feel time passing faster when we enjoy things that are rewarding or pleasurable, which increases dopamine activity in the brain. Losing time can also indicate dyschronometria (loss of time due to dyslexia, dementia, or certain parts of the brain being damaged), ADHD, or mental health issues such as depression.
On the non-medical side of things, losing time is often experienced when we become unaware of time passing as a result of being fully absorbed in an activity or task, a consequence of procrastination, a sea of distractions, having poor time management skills, having busy schedules, following a monotonous routine, lacking motivation, or even caught up in a few moments of unplugged mindful bliss.
Another common way of tracking time is birthdays, the celebration we embrace that says we have managed to survive the trials and tribulations of another passing year. I recently celebrated my 50th birthday, 5 decades, or a half of a century depending on whether it is laden with jokes or not.
Another way of marking milestones of time is by recognizing certain anniversaries. Some anniversaries are endured (usually those associated with heartache, sense of loss, or grief); and some celebrated (like a birth, graduation, marriage, accomplishment, or milestones).
This brings us full circle to what is spurring the creation of this Blog today. This year marks the 10 year Anniversary of the very thing that inspired this very blog – an auto accident on January 4, 2014. I have posted a blog every year on or around this Anniversary, with the exception of last year (the 9th year). I was prepared to write one and then as each day passed it became something I felt I had to forego as the words I envisioned putting here seemed too far out of reach. This year, I genuinely wanted to post this on the 4th yet as the 4th got closer and closer I started to feel some kind of absolute obligation to acknowledge how far I have come. 10 years, after all, is a hell of a milestone.
I kept sitting with the words, thoughts, experiences, and memories, or lack thereof, swarming in my head of the last 10 years of this recovery and rehabilitation journey; a journey where I have inherently made, and continue to make, valiant steps at re-inventing myself. I am slowly blossoming into the me I have been becoming, and it is ironic how things have come full circle, and I am left with a stark realization that I have been gifted with time. This whole process has been extensively mind boggling, emotionally mercurial, and fills me with pause.
Let’s make a full stop to digest that for a moment.
There are many events, lessons, personal developments, professional developments, and a sordid amount of moments that have taken place. The list would be impossible to delineate or detail in a simple blog post. Yet, all have been consequential to my growth as a human being with all the cloaks of comfort and opportunity I wear (as a mom, wife, sister, friend, survivor, student, advocate, business owner, etc).
I will take this opportunity though to turn the hourglass into a verbal synopsis. Pain still wreaks havoc with me, often very unpredictably, though is more managed. Mobility is still a challenge in lots of ways, and in some ways I see, declining, yet I am still mobile, breathing, functioning. This is worth celebrating. Finances are an ongoing real struggle, yet we still find a way to make things possible. I am sure this is due to a lot of divine intervention and is truly a miraculous feat in and of itself. I am currently safe in a home with my family, and in a Country with amenities we would not be afforded in other Countries, and for this I am deeply grateful. My memory and emotions are all over over the place – each like a new discovery that I continue to protect and covet. My health is a rubik’s cube that occasionally lines up, and other times is a series of rotating puzzle pieces. However, I am still able to think, research, learn, and evolve.
I have a deep appreciation for the linked together moments that build on each other. I have been enjoying the last 3 years as a new grandmother. We now have 3 grandchildren. We have lived to see only 2 boys left at home, our youngest start High School, and I myself have even returned to school to further my own education. I have met many professional goals (albeit much slower than I originally envisioned), and continue to move forward with this venture. We have all been blessed with 9 more years of time with my mom (who nearly died, went on and came off a vent in 2015). Indeed, there are many things to be grateful for.
My journey has afforded me the opportunity to network, meet, and advocate with lots of providers, organizations, individuals, and groups that I may not have had the opportunity to know without the time that I have been given.
This is what guides me and propels me in a forward thinking fashion. Seeing the precious process of experiences, creating new memories, and choosing to navigate all things given – whether effective or ineffective in my life.
As time passes, and I continue to reminisce about the last 10 years, and what the next 10 years might hold, I continue to be wrapped in the warmth of HOPE, faith, and an ever present growing awareness of my own mortality.
Until then….we celebrate! We celebrate being 50 years young. We celebrate only being halfway to reaching a century. We celebrate not only surviving, but thriving! We celebrate those moments that build into additional moments, which build into – despite any disabilities, hurdles, struggles, or setbacks – a life worth living.
~Caren Robinson, January 2023
I look forward to hearing your feedback. There are a number of ways to connect.
Happy 10th Anniversary to me and all my fellow HOPEsters!
Hello our fellow HOPEsters. We are glad to be entering this New Year of 2024 with all of you. We are thrilled to share with you that a series of new releases of pages, blogs, and updates on our Site has begun.
Check out our updated tabs across the top of your page when you arrive at our Site. Check each one carefully as some of them have dropdowns that lead to other pages. There have been a few adjustments and a few additions we are sure you will find useful.
Check out our 3 newest page releases done this week:
What in the world is this comment about sex being the “final frontier”? Okay, let me explain.
We are not talking about Star Trek here, though its reference to “Trekkies” is well known. The “final frontier” references space and how space is truly massive. It is estimated that the Universe is 100 billion light years across and still expanding. It’s “final” because it is assumed that our species (as humans) will never survive long enough (in our current form) to explore it all; it means that the voyages of outer space are continuing as we explore and discover strange new worlds; seek out new life and new civilizations.
What does any of this have to do with sex you ask, or removing its stigma? It can seem quite daunting learning all there is to know about sex. There is so much to learn about the body. We are still making discoveries, gaining knowledge, and opening up new opportunities for awareness as time marches on. We are only just beginning to discover how our brain and bodies are connected, how hormones change, how gender differences and other forms of trauma affect rehabilitation and healing processes; and how best to nurture neuroplasticity. We are just touching the surface of how our bodies change during and after trauma. I am certain this will be a discussion that continues as science and studies evolve. However, now, in this moment – let’s get back to the topic at hand.
What’s not to love about feeling good and enjoying feel good touch, closeness, intimacy, and unbridled pleasure? Some may refer to this experience as being “turned on”. However, what happens when that getting “turned on” experience stops working and suddenly becomes mysteriously illusive by getting “turned off”.
I became interested in this topic in the quest for exploring my own experience with my own sexuality changes after being struck with a polytrauma and traumatic brain injury as a result of a 2014 motor vehicle accident. Consensual sex has been an incredibly important and enjoyable part of my development as an individual, a woman, and as a wife. When I first started having sex I found it to be quite pleasurable, and a treasure hunt of sorts to new lands of awkward fumbling, exploratory kinks, taboo experimentation, joyful and explosive orgasms, and body riveting transcendent experiences. My libido was….what I assumed… normal. However, later I would learn when comparing with my other female friends, quite a bit higher than most of my counterparts. What can I say?….I loved sex and all the things that came with the consensual experience. I think sometimes, my desire outweighed the interests of my partner and that could get complicated sometimes. We always found the humor in it – that is, until the accident.
After the wreck, so many things changed about my body. I had…and still have, so many things going on, on so many levels. I was dealing with orthopedic injuries, multi-system issues, endocrinological changes, difficulty breathing as a result of injuries sustained, a traumatic brain injury, cognitive changes, mobility issues, no libido whatsoever, and the sudden inability to do anything myself, including take care of my own body (dressing, bathing, etc) I also suddenly stopped having my menses (medically referred to as amenorrhea).
Okay, here’s some extra-extra that is a bit, you know, EXTRA! In the last 9 years (as of this writing anyway) of this rehabilitative journey, I have had my menses a total of about 4-5 times. On one hand, yay, no messes to contend with. On the other hand this comes with a whole host of potential medical cascading issues for the future – none of which are foreboding of good health and great times. In this part of my life, I continue to live on the precipice of a continual balance between fear and relief. I have not had a thriving and spontaneous libido during that whole time…probably less than the number of times I have had my menses. It sputters, it comes and goes, or just lies dormant just out of my reach and ability to find it. Talk about a mood killer. I couldn’t understand it. My mental interest and desire, and more often than not – lack of interest and desire, was not matching what my body was willing to receive or give in contrast to attempted experiences of the sexual part of me that seemed to be perpetually “turned off”. This dramatically affected me as an individual, a woman, and my relationship with my husband as his wife. God bless him – he has the patience of Job (bible reference there). This brought me to a serious hunt about, “what the hell was going on with my body, and why?” Surely other people had or were experiencing this same strange phenomenon. Guess what? I discovered in my research…that they were! Why did I have to find out about this on my own instead of having this discussed as an important part of my rehabilitation plan by the medical professionals who should have been educating me? I had so many questions!
This blog’s proposed focus is to discuss the relationship changes that take place in the intimate aspects of a relationship after brain injury and trauma. One of the many questions I let guide my research was what changes can happen regarding intimacy and sex after a blunt trauma and what are some ways to adjust to those changes? Another question was how can we normalize talking about sex, identify any changes in the sexual aspect of a person’s life, and the importance of one’s sexual identity as part of the healing process or the rehabilitation plan after a trauma? How can we address the stigma that individuals with disabilities or mobility issues are not human beings with desires, needs, and an interest in that part of their lives?
I am hoping that the blog will accomplish opening up a dialogue about a seemingly taboo topic, rarely even discussed by healthcare professionals with their patients. I am hoping that it will help “normalize” the conversation about sex, our understanding about how sex affects our health, and how a person can manage any changes they may be experiencing after having a change in the way they engage sexually with their partner after a trauma. Viewing sex as an important topic in a rehabilitative care plan along with the other body systems, is worth addressing.
Brain injury is a growing health care crisis in our Country as is the awareness of mental health issues. Changes in intimacy/sexual relationships is quite common after brain injury, yet this isn’t widely discussed. A person’s body goes through numerous endocrinological changes that can affect libido, ability to perform, etc.
Common characteristics for persons with moderate traumatic brain injury include long and short term memory loss, being easily distracted, quickly angered, inability to solve problems, get tired quickly, and difficulties with sexual desires (Sica, 1996).
Many patients with brain injuries report physiological sexual disturbances and decreased sexual ability (Kreuter M;Dahllöf AG). Women with traumatic brain injuries (TBI) have been historically underrepresented in clinical research. Compared to the sexuality of women with neurodisabilities, male sexual problems and treatments are better documented (Bell, K. R., & Pepping, M.) Based on this high level of commonly reported changes as a result of a traumatic brain injury, it is important to inform patients about possibilities of optimizing their sexual ability. Programs organized to provide sexuality education should be an integral component of TBI rehabilitation. (Kreuter M;Dahllöf AG)
Sexuality, even before brain injury, is one of the most complex aspects of life. Sexuality can be seen on the pyramid in the hierarchy of needs for every human being since physical touch, intimacy, and love are an important and essential part of not just living life, but having quality of life as part of that existence. This is further evidenced by the works of Maslow.
In Maslow’s Hierarchy of Needs Theory, the specific needs are listed in detail in a hierarchy of needs pyramid (Maslow, 1970). Maslow’s Hierarchy of Needs is used today for assessing a person’s quality of life (Collins, Lanham, & Sigford, 2000). Health-related quality of life is affected by the person’s physical health, psychological state, level of independence, social relationships, and how these factors combine with one’s environment (World Health Organization)
Maslow developed five levels of the hierarchy of needs; physiological needs, safety needs, love needs, esteem needs, and self-actualization needs (Maslow). The bottom two levels are physiological needs and safety needs which, together, make up basic needs. Physiological needs are biological in nature. For example, the needs for oxygen, food, water, and a relatively constant body temperature are parts of physiological needs. These needs are the strongest, because if the person does not satisfy these needs, then the person would die. Safety needs are the establishment of stability for oneself. Next are social and esteem needs—also referred to as psychological needs. Love and belongingness are the needs to help escape loneliness and alienation and causes a person to have a sense of belonging and a sense of being loved. Esteem needs have to do with people needing a stable high level of self-respect, and respect from others. Self- confidence and feeling valuable are also part of this level. If these esteem needs are not met, the person feels inferior, weak, helpless and worthless. Self-actualization needs are at the top level of Maslow’s pyramid, and someone who is self-actualized is said to be at (or in the pursuit of) their full potential. The need for self-actualization is the desire to become more and more what one is, to become everything that one is capable of becoming. The person who has all the other needs can maximize his or her potential (Maslow, 1970).
Sexuality, while complex, becomes even more complex when you add to it, damage from an injury or trauma that causes changes to that quality of life. Brain injury can directly and indirectly affect important aspects related to sexuality and sexual function. (Moreno JA). To date, there seems to be no study that addresses the possible interventions that can improve awareness of deficits and perceptions of quality of life of persons with traumatic brain injury.
Specifically, examining whether interventions can successfully improve perceptions of quality of life and awareness of deficits are not often seen in the literature. (Chandrashekar, R. 2005)
A brain injury commonly alters sexual functioning as well as desire. It causes a decreased ability to achieve an erection, decreased ability to experience orgasm, decreased sexual desire and diminished frequency of intercourse. A high degree of physical independence and maintained sexual ability were the most important predictors for sexual adjustment. (Kreuter M;Dahllöf)
Two Types of Brain Injury
There are two types of acquired brain injury: Traumatic and Non-Traumatic
The first and most common is called a Traumatic Brain Injury (TBI). A traumatic brain injury (TBI) is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force. Traumatic brain injuries are defined as closed (or non-penetrating), or open (penetrating).
Injuries from sports or during combat (such as blast injuries from explosions)
Severe head injuries usually result from crushing blows or penetrating wounds to the head. Such injuries crush, rip and shear delicate brain tissue. This is the most life threatening, and the most intractable type of brain injury. TBI can also cause epilepsy and increase the risk for conditions such as Alzheimer’s disease, Parkinson’s disease, and other brain disorders that become more prevalent with age.
Repeated mild TBIs occurring over an extended period of time (i.e., months, years) can result in cumulative neurological and cognitive deficits. Repeated mild TBIs occurring within a short period of time (i.e., hours, days, or weeks) can be catastrophic or fatal.
The second type of non-traumatic brain injury is often called an Acquired Brain Injury(ABI). A non-traumatic brain injury causes damage to the brain by internal factors, such as a lack of oxygen, exposure to toxins, drugs, pressure from a tumor, etc. Examples of an ABI are:
Stroke
Near-drowning
Aneurysm
Tumor
Infection disease that affects the brain (ie: meningitis)
Lack of oxygen supply to the brain (ie: heart attack)
Drug Use
This blog specifically is focused on the research surrounding TBI’s, yet there are similar issues for those with ABI as well.
“Twenty percent of spouses/partners of persons with TBI reported sexual dysfunction, and 44% reported dissatisfaction with sexual functioning. Sixty-two percent of spouses/partners reported a decrease in sexual activity during the year postinjury, 34% reported a decrease in sexual drive or desire, and 34% indicated that sexuality was less important in comparison to preinjury. The sexual functioning of spouses/partners of persons with TBI was highly associated with the sexual functioning of the person with TBI. Age of spouses/partners and sexual functioning in persons with the TBI were significant predictors of spouses’/partners’ sexual functioning, even after controlling for sex of partners and the physical, cognitive, participation, and sexual functioning of the persons with injury”. (Sander AM;Maestas KL;Pappadis)
Rehabilitation professionals should provide education on the potential impact of TBI on sexual functioning for both persons with TBI and their spouses/partners, and integrate the assessment of sexual functioning into their clinical assessment, making appropriate referrals for therapy.
Where does our sexuality come from in our brains? “It is clear that frontal especially prefrontal lobe plays a role in sexual functioning as the cognitive functions are controlled by these areas and are significantly correlated with sexual functioning. The frontal lobe plays a valuable role in a person’s ability to plan, organize, emotional and behavioral control, personality, problem-solving, attention, social skills, flexible thinking and conscious movement. Injury to this area can cause problems such as inappropriate sexual behavior, difficulties with initiating sexual activity or difficulties with motivating oneself to engage in sexual activity. It can also cause difficulties with experiencing pleasurable and sexual sensations, spontaneity, and the build-up of arousal.
The temporal lobe plays a role in a person’s memory, recognizing faces, generating emotions, and language. Injury to this area has been linked to an increase in sexual interest and emotions (hyperactive sexuality), although it can also result in a reduced sex drive (hypoactive sexuality). Some people who have had temporal lobe injury have also been found to develop paraphilias (abnormal sexual interests that can sometimes be dangerous or illegal). Damage to pathways in the frontal and temporal lobes has been linked to difficulties in understanding whether someone else is interested in sexual contact, for example through body language and ‘reading’ emotions.
The parietal lobe plays a role in a person’s perception, spatial awareness, manipulating objects, and spelling; Wernicke’s area – understanding language; Broca’s area – expressing language. Seizures in this part of the brain can cause some brain injury survivors to experience sensations in their genitals, including heightened sexual arousal or sensations that are not pleasurable. For some survivors these sensations can even be irritating or painful.
The hypothalamus and pituitary gland parts of the brain are responsible for producing hormones in the body that regulate sex drive. Damage to these parts can therefore result in hormonal problems.
Brain injury is known to cause changes in thinking, behavior and body function which alters the way a person experiences and expresses their sexuality.
Changes to sexual behavior after brain injury could include erectile problems, reduced libido, the inability to orgasm, and the reduction in frequency of sex….or the increase and uncontrolled acting out of sexual behaviors/acts.” (Robinson, C. – 2021)
The following changes in sexual functioning can happen after brain injury in men and women alike:
“Decreased/Increased Desire: Many people may have less desire or interest in sex. Some people have increased interest in sex after brain injury and may want to have sex more often than usual. Others may have difficulty controlling their sexual behavior. They may make sexual advances in inappropriate situations or make inappropriate sexual comments, or vocal outbursts randomly.
Decreased Arousal: Many people have difficulty becoming sexually aroused. This means that they may be interested in sex, but their bodies do not respond to the touch felt that would normally stimulate sexual arousal. Men may have difficulty getting or keeping an erection. Women may have decreased vaginal lubrication (moisture in the vagina), or lack of sensation in the clitoral/vulva areas.
Difficulty or Inability to Reach Orgasm/Climax: Both men and women may have difficulty reaching orgasm or climax. They may not feel physically satisfied after sexual activity, or feel guilty for not coming to climax with their partner.
Reproductive Changes: Women may experience irregular menstrual cycles or periods.
Sometimes, periods may not occur for weeks or months after injury, or may stop altogether. They may also have trouble getting pregnant and develop signs of infertility. Men may have decreased sperm production and may have difficulty getting a woman pregnant.” (Robinson, C. – 2021)
This begs us to then ask questions about what causes changes in sexual function after brain injury? There are many, including some that are related to the brain itself. Others are
related to specific physical problems or changes in how a person may be thinking about sex or their relationships in general. Perhaps they have developed personality changes which have changed how they feel about the people they associate with.
There are many reasons sexual problems happen after someone has a brain injury. Some are directly related to the damage to the brain itself. Others are related to physical problems or changes in how the person is thinking about sex or relationships in general. They may also have had personality changes which causes them to change how they feel about the person(s) they are in relationship(s) with.
“Possible causes of changes in sexual functioning after Brain Injury include:
Damage to the Brain: Changes in sexual functioning may be caused by damage to the parts of the brain that control sexual functioning.
Hormonal Changes: Damage to the brain can affect the production of hormones, like testosterone, progesterone, and estrogen. These changes in hormones affect sexual functioning.
Medication Side Effects: Many medications commonly used after brain injury have negative side effects on sexual functioning.
Fatigue/Tiredness: Many people with brain injury tire very easily. Feeling tired, physically or mentally, can affect your interest in sex and your sexual activity.
Problems with Movement: Spasticity (tightness of muscles), physical pain, weakness, slowed or uncoordinated movements, and balance problems may make it difficult to have sex.
Self-Esteem Problems: Some people feel less confident about their attractiveness after Brain Injury. This can affect their comfort with sexual activity, their ability to perform, or their perception of how they may or may not perform.
Changes in Thinking Abilities: Difficulty with attention, memory, communication, planning ahead, reasoning, and imagining can also affect sexual functioning.
Emotional Changes: Individuals with brain injury often feel sad, nervous, or irritable.
These feelings may have a negative effect on their sexual functioning, especially their desire for sex.
Changes in Relationships and Social Activities: Some people lose relationships and friendships after brain injury or may have trouble meeting new people. This makes it difficult to date, build meaningful relationships, or find a sexual partner they are confident with, if they find one at all.” (Robinson, C. – 2021)
How do people with disabilities experience and engage with themselves as sexual beings? We have clearly established that while sexuality will remain a complex part of our lives, it has the potential to be greatly affected by brain injury and the cascading symptoms of that injury.
This cascade of symptoms can lead to dynamic changes to an individual’s ability to identify with their own sexuality in a familiar way and may change their outlook and experiences altogether. Sometimes these changes result in disabilities that may or may not be physically seen.
The sexual lives of people with disabilities have been disregarded and stigmatized. As a result, sexuality as a form of pleasure and an expression of love is not taken into account or even recognized for individuals with disabilities.
While one may concede that sexuality is a basic human need, awareness and knowledge about sexuality are shaped through a range of contextually specific sociocultural and religious ideas and practices. People with disabilities are systematically denied access to knowledge about sexuality, sexual behavior and services leading to their sexual marginalization. In addition to financial barriers and provider attitudes, other disability-specific barriers included relying on a known person, often a family member, to attend health clinics, which infringed their privacy and confidentiality. Enabling disability to be advanced at the national level in all development processes, would lead not only to young disabled people but also to non-disabled people receiving improved access to sexual health information, protection, and treatment.
“More than 15% of the world’s population are affected by disability, including physical and sensory impairments, developmental and intellectual disability, and psychosocial disability. While it goes without saying that people with disability have equal rights to sexual and reproductive desires and hopes as non-disabled people, society has disregarded their sexuality and reproductive concerns, aspirations, and human rights. People with disabilities are infantilized and held to be asexual (or in some cases, hypersexual), incapable of reproduction and unfit sexual/marriage partners or parents. The sexual and reproductive health and rights (SRHR) of people with disabilities continue to be contested, and there are particular concerns in relation to women with disabilities. For women, disability often means exclusion from a life of femininity, partnership, active sexuality and denial of opportunities for motherhood.” (Addlahka, R., Heidari, S., & Price, J.)
What also is not taken into account during the rehabilitative process, is the endocrine and physiological changes that can take place as a result of a brain injury, and the resulting changes that can occur in a person becoming oversexualized or on the other end of the spectrum, having a change of, or lacking libido, as a result of those changes. This can impact dating, marriages, and one’s own personal expression. Sexual expression is influenced by cognitive and emotional processes and is dependent on functioning anatomical and physiological systems, in other words, our brains control our sexual organs and responses.
As a human being, it is natural to want to experience pleasure, enjoy the company of another person, experience the touch of another person, and want to enjoy intimacy with your partner (or yourself for that matter).
There are some things though, that must be considered…..and an ongoing conversation that I encourage you to allow to take place…. Not only between partners, but with your provider as well…. BEFORE engaging in sexual activities after a head injury or sustaining any bodily changes that makes a person have newfound limitations, mobility issues, or disabilities.
Now, not everyone who has had a brain injury will have endocrine or sexual changes as a result of that brain injury. Not everyone that has a disability, mobility issues, or bodily changes has had a brain injury. Having a disability, whether caused by a brain injury or not, does not make us less of a person. We may have to get creative with how we have been used to experience sex, intimacy, and the human touch – do things differently…but that’s okay. (Robinson, C. 2021)
“Before resuming sex with a partner, boyfriend, girlfriend, or spouse, talk about it with your doctor or therapist and be guided by their advice. Make sure you are clear and talk with your partner about your expectations, fears, and feelings, including consent. Communication is key! Remember to not put too much pressure on yourself, focus on pleasure…. and not technique.
You may need to change your same old lovemaking style and experiment with other sexual activities or incorporating different things….which can include
oral sex and mutual masturbation
utilization of sexual aids/toys/furniture
to increase intimacy, concentrate on boosting the romance in your relationship by offering lots of affection, complimenting and saying nice things to each other and celebrating big and small occasions.
After a brain or body injury, it is just as important for you to protect yourself from unplanned pregnancy and from sexually transmitted disease as it was before your injury. Even if a woman’s period has not returned, she can still get pregnant. Even if she is having her period, she can still get pregnant. Here are some tips to help with birth control and protection from sexually transmitted disease.
Do research to help figure out what method of birth control and protection from sexually transmitted disease are best for you.
Because of changes in thinking abilities, it may be harder for you to remember to use protection or to remember to take it with you.
You can plan ahead by always carrying a condom or other method of protecting yourself and your partner.
For women who use birth control pills, or a device that must be replaced, using a calendar or alarm on a smart phone can help you remember to take the pills or change the device.
If you are unsure whether your partner has a sexually transmitted disease or has been intimate with others who have such disease, it is safest to use a condom.
If you have engaged in any risky sexual behavior, one of the best things you can do for yourself is to get tested for sexually transmitted diseases and get treated if you test positive.
Consent should not be assumed
“Each of us is responsible for making sure we have consent in every sexual situation. If you are unsure, it is important to clarify what your partner feels about the sexual situation before initiating or continuing the sexual activity. Consent should not simply be assumed by
Age: Age of consent is a legal term for the age a person must reach to give consent to sex or sexual acts. If an adult engages in any sexual acts with someone below the age of consent, they are committing a crime called Statutory Rape.
Also, just because someone is legally of age to consent to sex in your State/Country, does not mean they are mentally competent to consent. Someone may be considered incapable of consent if they are physically, mentally, or developmentally disabled, including….for example….a Senior, with Dementia.
Body language, Appearance, or Non-Verbal Communication: One should never assume by the way a person dresses, smiles, looks or acts, that they are consenting to, or want to have sex with you.
Dating relationships or previous sexual activity: Simply because two or more people are dating or have had sex in the past does not mean that they are consenting to have sex with you.
Marriage: Even in marriage, a person should not assume they have consent for sexual activity. Marital rape is as serious as any other sexual assault. Consent is required in all relationships, including married ones.
Previous Activity: Consent to engage in one sexual activity at one time is not consent to engage in a different sexual activity or to engage in the same sexual activity on a later occasion…even if it is on the same day.
Silence, Passivity, Lack of Resistance, or immobility: A person’s silence should not be considered consent. A person who does not respond to attempts to engage in sexual activity, even if they do not verbally say no or resist physically, is not clearly agreeing to sexual activity.
Incapacitation: A person being in a coma renders that person incapable of giving consent. Someone who is in a coma is unconscious and has minimal brain activity. They are alive but cannot be woken up and show no signs of awareness. They are essentially unresponsive to their environment. Sex with someone in a coma is considered RAPE. Plain and simple. Other incapacitation can happen when Alcohol consumption or use of other drugs (even if those are their own prescription drugs) can render a person incapable of giving consent. Alcohol, sometimes drugs, and even a combination of the two is often used as a weapon to target individuals ….and is used by perpetrators, to excuse their own actions. This is not excusable.” (Robinson, C. – 2021)
Additionally, while all states have their own specific laws – here in Michigan….the Criminal Sexual Conduct laws apply to a perpetrator regardless of whether or not they were drinking. It is important to remember that sexual assault is never the survivor’s fault, regardless of whether they may have been intoxicated or not.
The term “sexual assault” means any unwanted, nonconsensual sexual contact of any kind (including kissing) obtained through the use of force, threat of force, intimidation, or coercion.
“Rape is unwanted, non-consensual sexual contact that includes penetration (i.e. vaginal or anal penetration, oral sex, and genital touching) obtained through the use of force, threat of force, intimidation, or coercion. 80% (8 out of 10) of all rapes and sexual assaults are reported to be committed by strangers, which means that most of these crimes are committed by someone the victim knows, is close with or related to”. (according to RAINN).
Now that we discussed all the serious business about Sex, Consent, and being aware of our responsibilities around sex….let’s dispel some myths about disability and sex….
Myths About Disability and Sex
Disabled people can’t have sex.
Disabled people must pay for sex.
Disabled people aren’t sexy.
Disabled people don’t want or need sex.
Disabled people only have kinky sex.
Disabled people only have sex with other disabled people.
Disabled people can’t have kids.
Disabled people cannot enjoy or are not interested in sex if they are paralyzed.
Disabled people shouldn’t have kids because they can pass on their disability.
If you have sex with a disabled person, you will catch what they’ve got
Disabled people are a burden on their partners.
People living with a disability can’t have “real” sex.
Disabled people need protection, like kids.
Disabled people have more important things than sex to worry about
Disabled people are brave and courageous to try sex (no, it’s just adapting to a new lifestyle….this does not make them brave – it makes them humans with sexual needs….like anyone else).
All persons in wheelchairs, using walkers or canes are chronically ill, frail, or sickly.
Facts About Disability and Sex
People with disabilities can be sexual and enjoy sex.
Some people who use a wheelchair, walker, or can still feel “down there”
Sex is not just all about each other’s “privates”, it’s about intimacy as well
People with disabilities can be kinky and sexy.
Mobility aids can be a fun addition.
People with a physical disability don’t always just “lie there”.
Disabled people can have sex and enjoy it.
Disabled people sometimes choose to pay for sex like people who aren’t disabled.
Disabled people can enjoy the same sexual experiences as those without disabilities.
Disabled people can have sexual desires/needs.
Disabled people can have kids and build families of their own.
People with disabilities can identify as LGBTQ too.
All people need to learn about and understand sex.
Conclusion:
There is a silence within society that pervades many areas of disability and sexuality resulting in the views of disabled people being rendered absent or invisible. Ideally this will open at the very least, a dialogue to inform disabled and non-disabled about people’s sexuality after trauma (regardless of how a person identifies themselves) and empower them in the social and sexual choices they make.
A patient’s ability to cope with a change in brain function post-TBI has been shown to be an important factor in recovery and outcome (Anson and Ponsford, 2006). Articles like this make it possible to make it less of a taboo topic and bring more awareness that encourages providers to include a discussion about sexuality as part of the rehabilitation process.
Rehabilitation professionals should provide education on the potential impact of TBI on sexual functioning for both persons with TBI and their spouses/partners, and integrate the assessment of sexual functioning into their clinical assessment, making appropriate referrals for therapy. (Sander AM;Maestas KL;Pappadis)
Yes, sexuality is one of the most complex aspects of life but, the sexual lives of people with disabilities have been disregarded and stigmatized for far too long. We have the ability through education and awareness to remove those stigmas and make sexuality a normal part of conversations, not just with our healthcare providers, but with each other as well.
There is a way to breathe life back into having moments of being “turned on” when you have unexpectedly been “turned off”. It may feel like a betrayal by your body to not cooperate with you the way it used to before your brain injury. It may look different than it used to. It will, I promise, feel different than it used to. However, as time goes on, and healing continues to work its way into new synaptic connections and your body re-routes itself – you may have the opportunity to experience blissful levitations and waves of sporadic pleasure…. even if for just a moment. This creates a feeling of hope and gratitude that the seemingly robotic new form of yourself is still human after all.
Sex and Disability…..the correlation is a powerful necessary talking point. We must remember when dealing with this level of dis-ability as a result of a brain injury or trauma, not to dis…. our abilities. Let’s boldly go where no man….or woman has gone before! We must continue to keep the conversation, exploration, and research going forward to help remove the stigma and normalize the approach to sex after brain injury and trauma.
Anson, K., and Ponsford, J. (2006). Coping and emotional adjustment following traumatic brain injury. J. Head Trauma Rehabil. 21, 248-259.
Bell, K. R., & Pepping, M. (2001, February 12). Women and traumatic brain injury. Physical medicine and rehabilitation clinics of North America. Retrieved from https://pubmed.ncbi.nlm.nih.gov/11853035/
Bryant, R.A., and Harvey, A.G. (1999). The influence of traumatic brain injury on acute stress disorder and post-traumatic stress disorder following motor vehicle accidents. Brain Inj. 13, 15-22.
Collins, R., Lanham, R. A., & Sigford, B. J. (2000). Reliability and validity of the Wisconsin HSS Quality of Life Inventory in traumatic brain injury. Journal o f Head Trauma Rehabilitation, 15, 1139-1148.
Kreuter M;Dahllöf AG;Gudjonsson G;Sullivan M;Siösteen A; (n.d.). Sexual adjustment and its predictors after traumatic brain injury. Brain injury. Retrieved April 13, 2023, from https://pubmed.ncbi.nlm.nih.gov/9591141/
Lezak, M. D., & O’Brien, K. P. (1988). Longitudinal study of emotional, social, and physical changes after traumatic brain injury. Journal o f Learning Disabilities, 21, 456.
Maslow, A. H. (1970). Motivation and personality. New York, NY: Harper & Row.
Moreno JA;Arango Lasprilla JC;Gan C;McKerral M; (n.d.). Sexuality after traumatic brain injury: A critical review. NeuroRehabilitation. Retrieved April 13, 2023, from https://pubmed.ncbi.nlm.nih.gov/23422460/
Rape, Abuse & Incest National Network) is the nation’s largest anti-sexual violence organization. (2023). Perpetrators of sexual violence: Statistics. RAINN. Retrieved from https://www.rainn.org/statistics/perpetrators-sexual-violence
Reekum, R. V., Cohen, T., & Wong, J. (2015, January 24). Can traumatic brain injury cause psychiatric disorders? Can Traumatic Brain Injury Cause Psychiatric Disorders? Retrieved from https://neuro.psychiatryonline.org/doi/10.1176/jnp.12.3.316
Sander AM;Maestas KL;Pappadis MR;Hammond FM;Hanks RA; ; (n.d.). Multicenter study of sexual functioning in spouses/partners of persons with Traumatic Brain Injury. Archives of physical medicine and rehabilitation. Retrieved April 13, 2023, from https://pubmed.ncbi.nlm.nih.gov/26845190/
Sica, R. B. (1996). The neuropsychological basis of potential co-occurrence of mild traumatic brain injury with posttraumatic stress disorder. [Electronic version] Trauma Response, 5(2), Article 6.
World Health Organization (1998). Life in the 21st Century: A vision for all. (World Health (Rep.) Geneva, Switzerland: Author.
What is the correlation between faith and hope, and what exactly is a miracle as it relates to hope and faith?
Compiled By: Caren Robinson
”The whole world is a series of miracles, but we’re so used to them we call them ordinary things”
~ Hans Christian Andersen
My current connection to this topic is originated from being raised in a faith based home; exploring/educating myself about multiple religions over the course of my life, and life experiences that have shaped my view on each of these concepts.
I already know this is a controversial topic because there are so many beliefs, strong opinions, and non-believers, that I risk alienating someone with my writing, or not connecting with my audience. This was also spurred by the experiences I have had since recovering from a catastrophic car wreck with my youngest son and a series of traumatic life events. This near death experience forced me to face everything I knew to be true and examine that which I didn’t know or understand as well. It conjured up pieces of complex opportunities that I would not have been given were I not to live through these experiences.
I know that this piece will challenge perceptions, and ideally I will be able to present it in a way that is palatable and provokes thought.
What also draws me to this topic is the state of our Country; the global strife; the battle between being spiritual vs religious, vs science focused, vs a balance with some or all of those pieces; and my interpretation of the research done on these concepts and what that looks like. What draws me to this also involves what I have witnessed happen through different life experiences and unexplained events.
When beginning to explore this topic I had to ask myself in a really direct manner – how can I make this unique, novel, personal, and not rehash what has already been said or spoken numerous times before but just in different formats?
I went on a hunt to be able to at first define what faith, hope and a miracle was. Then I began to really immerse myself into how they correlated. Anyone seeking to cope, anyone that believes in a power greater than themselves would benefit from this writing. Anyone, whether they were religious or not, whether they subscribed to a certain belief system or they didn’t – any of them would benefit and get valuable information from this writing. That was the goal and remains the goal throughout this blog entry.
So we begin with the dictionary definition of faith. We can find this in a number of dictionaries and while the definitions are similar, there is a lot of overlap. For this particular blog post though, I chose to utilize the Miriam-Webster dictionary.
Miriam-Webster dictionary defines “faith” as:
a: allegiance to duty or a person; loyalty b: fidelity to one’s promises
a: belief and trust in and loyalty to God; belief in the traditional doctrines of religion
b: firm belief in something for which there is no proof; complete trust; believe without question
a: something that is believed especially with strong conviction especially: a system of religious beliefs
Miriam-Webster dictionary defines “hope” as:
to cherish a desire with anticipation: to want something to happen or be true
trust; reliance
to desire with expectation of obtainment or fulfillment; expectation of fulfillment or success
to expect with confidence; someone or something on which hopes are centered
Miriam- Webster dictionary defines “miracle” as:
a: an extraordinary event manifesting divine intervention in human affairs
an extremely outstanding or unusual event, thing, or accomplishment
a divinely natural phenomenon experienced humanly as the fulfillment of spiritual law
I would identify myself as more of a spiritual person at this point in my life, rather than a religious person. Yet what does that really even mean? You may have heard a lot of folks now-a-days describe themselves that way. There is an even growing number of individuals who are breaking from the confines and walls of organized religion, or don’t even subscribe to any particular belief system who may still describe themselves as spiritual. Then again, you have that subset of individuals still who do not consider themselves religious or spiritual and yet still have faith, hope, and believe in miracles.
The majority of our society uses the words “religion” and “spirituality” interchangeably with the idea that they are the same things. However they are very different and have very different concepts.
“Religion is the rules, regulation, ceremonies, and rituals developed by man to create conformity and uniformity in the approach to God. Spirituality is God’s call in your soul.”
~ lyanla Vanzant
Religion is more external from ourselves and encompasses more of that institutional type of belief process. This is something that often involves a specific building with a structured belief system that contains members, converts, or pledges who practice certain rituals, beliefs, or practices. The fear of punishment for one’s actions is often a principle factor in religion. Religion simply involves a group of people who have common beliefs and faith about the divine. It is about adherence to rules, laws, and specific actions. Religion often discourages people from listening to their own instincts. In fact, most religions instruct and teach their “believers” to accept and do what they’re told, without questioning it; forcing them to stay fixed to a specific text, the scriptures, or whatever specific ideology they are being taught by their religious leaders.
Spirituality is really more internal and self-directed energy and essence that is more about one’s inner-self, soul, and personal development. A solitary experience of the divine that focuses on the individual experience, encourages the focus on individual energy, positive mindsets, and acts based solely on love; the ability to combine truths from various belief systems and apply those beliefs to their lives. Being spiritual entails maintaining one or more beliefs, adapting those beliefs based on personal study, self- reflections, interpretation, and the ability to connect with something greater than ourselves. Spirituality is very personal, and unique. It may involve some very sacred traditions, or practices; and yet, may be reflected in something as abstract as art, or our connection to nature or music. Spirituality encourages folks to do what they feel is right, despite the consequences.
Neither of these is better than the other and is truly a matter of personal preference – though there are plenty of people ready to fall on their sword defending one over the other, but that is not what we are here to discuss or argue in this blog post.
“Miracles are not in contradiction to nature.
They are only in contradiction with what we know of nature.”
~Saint Augustine
People that have hope, have faith. Seemingly, a person cannot have one without the other. Yet what is the correlation between them? There are many that would say that:
they have faith because they need hope
people have hope because they need faith
people have hope because they have faith
they have faith because they have hope
After all, “faith” expresses confidence in the truth, value, or veracity of someone or something and is often characterized by the absence of empirical proof that is not necessarily verifiable. Faith represents a belief that actually exists.
“Faith, in slogan form, is resilient reliance, by which we mean a disposition to rely with resilience in the face of challenges”
~Daniel Howard-Snyder
Then we have “hope”. Hope is directed to what will come, what is possible, toward the future…..of what may come. This may also be viewed as an anticipated fulfillment of a particular intention or focus.
According to Shannon Kincaid, Ph.D. and Philip Pecorino, Ph.D. from Queensborough Community College of The City University of New York – they state in one of their research papers that “…..one does not have to be an incurable optimist to claim that faith is a sufficient and necessary condition of hope. When people have hope they have faith, because they hold a belief that says “I believe that the future will be better.” And while they have no grounds to “prove” the hopeful assumption, they have faith in it. While faith without hope is possible, hope without faith is not. Thus faith is not sufficient for hope. Faith is necessary for hope but faith is NOT SUFFICIENT for hope because you can have faith about a number of things and yet no real hope. “
Then that brings us to miracles. Why do the vast majority of people not believe in miracles? This is possibly the direct result of living in a technologically science-driven and informational era where people are constantly demanding “proof” of everything and often, there is no “proof” of any miracles. No one has ever recorded, on camera, with no cuts or special effects, a leper being healed, a blind man being given vision, or anything even close, outside of medical advancement and treatment options.
Additionally, a lot of folks find it difficult to embrace or believe in something they cannot explain or cannot see. This is also why there is a falling away from organized religion to some degree because there is, to some individuals, no convincing evidence that God exists and if God doesn’t exist then surely miracles cannot exist. Yet, miracles, to me, are not a God-principle. Miracles are simply an unexplained event which absolutely defies, nature, physics, or any logical explanation. Then again, you can believe in supernatural events and not believe in God. Some would argue even that miracles are the result of confirmation bias, or coincidence, and impossible when it comes to the laws of Science and physics and often dismissed as falsities with those things that cannot be explained through a scientific process. The eighteenth-century Scottish skeptic philosopher David Hume argued, “the wise man should not believe in miracles”. The basis for his assertion was what might be called the “repeatability principle”— evidence for what occurs over and over (the regular) always outweighs evidence for that which does not (the rare). Since miracles are rare and contradict our uniform experience, Hume argues the wise man ought never to believe in miracles. While it’s true that a wise man should base his belief on the weight of evidence, it’s not true that evidence for uniform experience always outweighs evidence for what is singular and rare. Hume’s principle nullifies science itself. As an inductive discipline, science necessarily presupposes the possibility of discovering new things that may contradict uniform experience. It views rarity as that which disqualifies rational belief, yet rarity is of the essence of a miracle. Sure, it could easily be said that we need to exercise a heightened sense of awareness and sincere caution when confronted with accounts of the miraculous, however we should also be apt to following the evidence where it leads, even if we cannot explain it, no matter how extraordinary and improbable it is.
“… look for hope in a realistic way, and choose to lean in to it – but let it be part of the larger whole. You need not avoid the grief and distress that go along with the big picture. In fact, hope – or light – can be that much more exquisite and meaningful when it comes with full acknowledgment that darkness exists, too..”
~Dr. Andrea Bonlor PhD
Ultimately, we have control over the way we choose to believe. Whether we choose to have faith, hope, or believe in miracles even – or we choose not to believe in any of these. The belief or non-belief in and of itself seems to have a direct correlation to our actions. Since beliefs affect our behaviors, we have to step up and take responsibility for them. It is imperative to examine claims from all sides. It is imperative to examine claims from several different perspectives. It is imperative to be able to think on our own steed, and form our own conclusions based on our intuition and what we know to be true rather than simply accepting the opinions or forced beliefs of others. It is also imperative to be able to wrap our minds around the fact that not all things have an explanation. Not all things can be proven by Science. We are responsible for our beliefs because they are the consequences of things over which we do have control (for example paying attention to our prejudices, biases, or whether we choose to be open minded and curious; whether we choose to be religious or spiritual). Yet we have no control over the outcome or end result of a specific action or non-action because the Laws of the Universe often defy this.
These times that we live in they are uncertain. In a moment life can change. Everything we knew to be true can be catapulted and often is an immersive experience when thrust into unexpected life altering events. During these times, it is difficult to feel hopeful. There are plenty of studies to show that having hope for the future helps build our resilience – that ability to get through the seemingly impossible and recover more quickly. Hope can reduce stress, reduce anxiety, trauma, and depression. According to the “hope theory” formulated by positive psychologist Charles Snyder and his colleagues, hope gives people the will, determination, and sense of empowerment that allows them to reach their goals. Hope encourages emotional ownership. Hope reminds us of what we are working for or towards. Hope holds space and optimism for the future, keeps us committed to self-care, and ironically is science based. Let me explain. When a person has hope, it releases endorphins in the body and lowers stress levels. This increases mood, improves behaviors, and makes us more productive, even if the end goal or result seems illogical. Now hope is not the same as wishing either though. There is a profound difference between hoping and wishing. Wishing encourages passivity, whereas hope represents an active stance and actually taking action in a specific direction.
If I am focusing on a specific direction, a specific outcome, a desired result and I have hope, can I also have faith without being religious? I believe that we can. A lot of people are fed up with all the negative connotations and bad actions within various religious belief systems, churches, etc. yet they believe in a creator that is infinite and overall cannot be comprehended by anyone. After all, the human mind cannot quite seem to comprehend the infinite, which is why most people find it difficult to accept miracles as a possibility. While we may know, as a species, as people the meaning of infinite or vast….comprehending it is not something we have mastered. Not even with Science.
“Hope is a match in a dark tunnel, a moment of light,
just enough to reveal the path ahead and ultimately the way out.”
~ Dr. Judith Rich
Personally, I believe in God. I believe in the omnipotent power of the Universe. In a power or divine greater than myself. I believe in the Creator, even though I cannot fathom the form of the creator except that the creator is in the molecules and DNA of all things animated and inanimate. I believe that to be a Christian is to be “Christ-like” and that to be “Christ-like” means to embody that which is lovely, pure, and of good rapport. I believe that to be “Christ-like” means to treat others like you want to be treated. It means to be selfless, humble, confident, giving, charitable, and tolerant. I believe that embracing this form of belief is a culmination into one simple yet powerful word – FAITH. Yet I also believe that one can have Faith and not embrace any of these beliefs.
I can say with pure conviction that I would not have survived all that I have this far into my life without a strong connection to my Faith and a deep Spiritual Connection with something greater than myself. I can say that throughout the recovery process after the wreck I was in, there are times – when it feels – that all I have that is consistent, is my Spiritual self, and my every present life clinging grasp, onto HOPE.
I am not without humility when it comes to the fragility of life in general. I am truly in awe of the miraculous events, too numerous to be coincidental, involving that wreck and all of the circumstances in my life since. I truly believe that there were angel wings wrapped around my son that day. It is the only explanation for his survival….the only explanation for my survival. My continued courage to overcome seemingly insurmountable difficulties, medical and otherwise have only been conceivable due to my connection to God and the abiding Faith that I embrace. This propels me and gives me strength to never give up HOPE. I am not religious by any means. You may or may not have a tie to faith, hope, or miracles in your own life and your own experience. Yet I challenge you to keep an open mind and not to get bogged down on the things you cannot explain or prove. Sometimes you just have to know, to trust, and to make the best decisions you can. I also wholeheartedly believe in, support, and have a great and deep love for Science. Yet despite the laws of physics and all that comes with that line of thought, I am still faced with the unseen power of the topic of this writing.
There is indeed a correlation between faith and hope. There are indeed miracles that can happen as it relates to hope and faith and the belief that you give energy and power to.
S;, Griggs. “Hope and Mental Health in Young Adult College Students: An Integrative Review.” Journal of Psychosocial Nursing and Mental Health Services, U.S. National Library of Medicine, 1 Feb. 2017, https://pubmed.ncbi.nlm.nih.gov/28218927/.
We should probably start with defining intelligence. Intelligence can be defined as the ability to solve complex problems or make decisions with outcomes benefiting the that particular individual that involves problem-solving and decision-making. These are functions of the nervous systems, including the brain, so intelligence is closely related to the nervous system. There is not just one way to be intelligent or display intelligence. In fact they are 8 types of intelligence, with a 9th known as “existentialist intelligence” that has been recently introduced by Howard Gardner, a psychologist from Harvard. Gardner’s theory suggests that traditional psychometric views of intelligence are too limited.
What does brain injury look like? Do you know? What does someone look like who has a brain injury? Do you think of them as being unable to think anymore, or as a drooling incapacitated individual who has somehow lost their ability to be independent or do for themselves? What if they tell you they have a brain injury but nothing shows up on a CT Scan or an MRI – would you still believe them? What if someone didn’t start to have symptoms until years later? Do you think this is even possible or would you think symptoms should show right away? This writing is dedicated to any professional that works with or comes into contact with any person who may have sustained a brain injury.
I personally have had numerous concussions (brain injuries) throughout my life. I mean, anytime you hit your head and see “stars or sparkles” – guess what? That is a brain injury. That being said, I never gave a 2nd thought to them because I never had any seeming lasting damage or long term effects. Let’s face it, the education about concussions was not as advanced back when I was a kid, nearly 50 years ago. I mean, the fabric of education and discovery around medical science changes on a daily basis, and I am sure as a society we will continue to learn even more about our brains as time goes on.
When I sustained a closed head injury in 2014 my opinion about head injuries, what they looked like, and how they presented would forever change. In addition to multiple orthopedic fractures, I also had to overcome this new way of existing in a body I no longer recognized. I could not think the same way I used to. I could not pull up my words as fast. My recall was crappy and yet I still maintained the same level of intelligence as before my injuries, just the ability to process and trouble with memory made it near impossible to feel like I was able to express it in the same ways I was used to. Based on multiple accounts, certificates of merit, and other input given to me throughout my life, I was considered to be highly intelligent before all my injuries, so why after that accident was I now just testing as “average”. Why couldn’t I recall basic information, simple words, and struggle with putting my thoughts together? Why did my taste and smell and ability to be in crowds and around noise change?
Noone professional, or in roles to educate me on this really seemed concerned about this at first. Just me. They would say things like, “you communicate really well so you’ll be fine”, or “most of society is average so you are good”, or “you should be happy you aren’t worse”, or “everybody gets headaches or forgets things”. They weren’t listening, only getting caught up in the numbers of the “average” of their other patients – not dealing with me as an individual or taking my concerns, or the concerns of my family seriously. I was worse – they just couldn’t see it. “Great”, I told myself, “I am happy for everyone else, but this is not normal for me”.
How could these providers look me in the face and say I was fine, especially since they didn’t even know me before my injuries? How could they be so callous, indifferent, and lack basic knowledge in a field where they should be teaching me about these changes?
I knew I was different. My family knew I was acting different. The me I used to be was gone. Killed in that accident. I was now living with a stranger in my body. I knew my thinking and processing and memory was off. It was a daily and sometimes moment to moment battle. Yet since I was suddenly “average” I was okay to those looking at the data and my life. I was not average to myself. I was falling apart and while different than those fractures in my body I also sustained and everyone could see, my brain injury they could not see. My injury remained invisible on a regular MRI and CT scan since I didn’t have a skull fracture or hemorrhage. Apparently the general thought was that the brain swelling that encapsulated my brain and then reduced made me all better. False! In fact, I was generally dismissed as just needing to be patient and give myself “time to recover”.
Then the most miraculous thing happened. I discovered in my search a special brain scan called a SPECT CT (different than a regular CT scan). Michigan No-Fault was a lifesaver in providing me the opportunity to get this scan done. The SPECT CT, which showed diffuse axonal shearing in multiple parts of my brain….finally PROOF…something that could be “seen”. Honestly, that test was a game changer in a lot of ways….but that is another story.
Let’s start here though and focus on what this writing is about to begin with. You can be highly intelligent, experience a brain injury and still be highly intelligent. This is what confuses people who see you and interact with you. To them, you are still “normal”. A brain injury does not necessarily affect intelligence. Intelligence is a stable trait which includes many aspects of cognitive functioning. Following a traumatic brain injury, the brain is unable to function as well as it did prior to injury. This is why we typically see some difficulties with memory or academics. However, once the brain recovers there is no change in a person’s overall intelligence. Your intelligence is based, depending on the definition of intelligence, on the sum total of your knowledge.
Someone’s IQ can be unaffected by a TBI, but other parts of the brain that “pilot” or guide one’s brainpower can be messed up. Decision-making and complex social interactions can cause major problems in one’s life and career. The individual with high intelligence may still have cognitive problems such as headache, difficulty thinking, memory problems, attention deficits, mood swings and frustration. These injuries are commonly overlooked, especially in those with high intelligence. Their low threshold of functioning or slower processing speeds may appear as average where prior to injury they would have tested as above average.
Something interesting I discovered in my studies is that the brain of the intelligent person is more complex in appearance, not as soft, and has greater weight relative to size. Additionally, it can be noted that the intelligent brain may have an enlarged prefrontal cortex or parietal lobe relative to other areas of the brain. More intelligent people have more wires, more connections and more complex architectures in their brains. These are reflective of genetics, as well as developmental experience. Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.
That being said, Intelligence and personality dysfunctions after minor traumatic brain injury (TBI) (whiplash; slight head impact) incurred in a motor vehicle accident (MVA) were studied in adults after an average interval of 20 months. There was a mean loss of 14 points of Full Scale IQ from estimated preinjury baseline IQ determined from the standardization group (WAIS-R) without evidence for recovery. Personality dysfunctions included cerebral personality disorder, psychiatric diagnosis (30 of 33 patients), post-traumatic stress disorder, persistent altered consciousness, and psychodynamic reactions to impairment. Cognitive loss is caused by interaction of brain injury with distractions such as pain and emotional distress. Unreported head impact and altered consciousness at the time of accident contribute to the underestimation of brain trauma after minor TBI.
I can tell you this. There is a saying in the brain injury medical community that if you have seen one brain injury, you have only seen one brain injury because no two brain injuries are alike. While there are many symptoms that are consistent with each other and may overlap between folks, there is one thing you can be sure of – it is consistently inconsistent.
In fact, there are a lot of misdiagnoses for ADHD, ADD, and ODD when instead these folks should be screened for history of brain injury and have neuro testing done as well before making a blanket diagnosis. Now this doesn’t mean that all people diagnosed with ADHD/ADD are misdiagnosed. However, it does mean that if they have a history of a brain injury it is something worth exploring.
Unless there is objective evidence (evidence you can physically see that is obvious) of brain injury on MRI or CT Scan (hemorrhages, hematoma’s penetrating skull fractures into the brain, etc) people (including uneducated providers) assume the individual expressing symptoms of a traumatic brain injury may be faking, exaggerating, or malingering their injuries or the person has psychological problems that had to have pre-existed before their accident. The reality is that the majority of mild (mTBI) and moderate brain injuries show normal results on an MRI and CT scans. That’s right, you cannot see the injury with these particular tests – and a lot of folks develop psychological changes and personality changes as a result of their injuries.
The basic imaging of an MRI or CT Scan also does not show diffuse axonal injuries nor do they show levels of intelligence.
Keep in mind also when working with your patients, clients, or colleagues, that women also tend to have longer recovery times than men with regard to brain injuries as shown in recent studies. Recent studies on women’s brains finally coming to the front of the class in the scientific community. This is important because almost all research has previously been done on just men’s brains.
We are learning that there is damage we can’t see with the naked eye that requires special testing (like a SPECT CT) and that is called diffuse axonal injuries (DAI). Someone with diffuse axonal injuries may also have brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Which by the way, does not necessarily affect the person’s intelligence.
Diffuse axonal injuries (DAI) are caused by acceleration, deceleration, and contact forces. DAI affects individual nerve fibers which can lead to a disruption in nerve communication. DAI is microscopic damage to the axons in the brain neural tracts, corpus callosum, and brainstem, is associated with significant mortality and morbidity. When these forces are great enough it creates a shearing force that severs the axons of nerve fibers, which causes nerve cells to die and can create swelling in the brain. The main symptom of diffuse axonal injury is lack of consciousness, which can last up to six hours or more. A person with a mild or moderate diffuse axonal injury who is conscious may also show other signs of brain damage, depending upon which area of the brain is most affected. Diffuse axonal injury causes cognitive, physical, and behavioral changes that compromise social reintegration, return to productivity, and quality of life of patients and their families. These changes persist beyond the acute phase of treatment and continue for a long period after the traumatic event. Diffuse axonal injury, and more generally TBI, often results in physical, cognitive, and behavioral impairments that can be temporary or permanent.
Due to the diffuse and microscopic nature of the injury, CT scans and general MRIs are typically negative unless small areas of bleeding within the brain are noted within the cerebral cortex or corpus callosum (tracts of white matter in the brain). If a patient presents with unconsciousness and these tests are negative, the medical facility should move onto a different imaging technique to check for DAI. Depending on the severity of the injury and the extent of the damage. A concussion can be considered a mild case of shearing brain injury. At its mildest, DAI can occur unnoticed.
Another thing for providers to be aware of when dealing with their patients, clients, or colleagues is that tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.
The bottom line here is that you can’t get tunnel vision and just assume that because your patient looks okay, that they are okay. You should keep in mind that a patient knows themselves better than you know them. If they are telling you that something is wrong and they are different – then listen and take that seriously.
If a person has a brain injury with long lasting debilitating symptoms, they can still have the same intelligence. You can have a severe traumatic brain injury with empirical radiological evidence of damage and still maintain your intelligence. Brain injury does not equal lack of intelligence. A person’s intelligence is not a solid basis for deciding a person’s extent of disability after an injury.
What I hope you get out of this is a way to relate to, offer help for, and be better informed about brain injuries so you can offer the best possible care to the people you work with.
The High IQ TBI (a blog which is worth the read about high IQ and TBI – this will take you to a different site)
References:
RS, P. and A, R., 2022. IQ loss and emotional dysfunctions after mild head injury incurred in a motor vehicle accident. [online] PubMed. Available at: https://pubmed.ncbi.nlm.nih.gov/8682910/
Vieira, R., Paiva, W., de Oliveira, D., Teixeira, M., de Andrade, A. and Sousa, R., 2016. Diffuse Axonal Injury: Epidemiology, Outcome and Associated Risk Factors. [online] National Library of Medicine. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5071911/
Wood, R. and Rutterford, N., 2006. Long-term effect of head trauma on intellectual abilities: a 16-year outcome study. [online] National Library of Medicine. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2077538/
Gao, MD, PhD, B., Jiang MD, S., Wang MD, PhD, X. and Chen MD, J., 2000. The Role of Pre-injury IQ in the Determination of Intellectual Impairment from Traumatic Head Injury. [online] Neuro.psychiatryonline.org. Available at: https://neuro.psychiatryonline.org/doi/pdf/10.1176/jnp.12.3.385
Due to growth in our submissions, we took this opportunity to split up one of our pages into 2 different pages for your convenience.
Our original page used to be called Support Groups Sites and Books. This link will no longer work. However, we still have all of the great resources from this page now split into 2 pages.
Did you learn something, read anything that inspired you, or impacted you on this Site? Do you support bringing awareness to the topics written about on this Site and want to see more content?
Keep This Website active, growing and it services FREE.
You can support general operations, outreach, and awareness efforts of HOPE TBI.
Hello my fellow HOPEsters. I am so very excited to introduce and offer some additional and new opportunities and resources to bring awareness about brain injury and polytrauma to our followers, supporters, advocates, and new HOPEsters on a global level
Can you believe we have been around for 8 years now?
While we will continue to offer all of you many free resources here at HOPE TBI, including relatable content through an active Blog, numerous resources, our tireless research on various topics, an evolving informational podcast, networking opportunities, and help in creating and e-publishing your stories – we are now also offering some other additional options as well.
We are now able to offer informational workshopstailored for your organization, group, class or event.
We also are now able to offer supportive services at an elevated level through our new medical advocacy consultant services with monthly memberships. at a considerable and affordable option for those interested in a bit more than what we offer for free.
Check out our paid services pageunder the “About Our Site” tab at the top of the page on the left (first tab on the menu list if looking at this from your mobile).
Let us know what you think check out the page and let’s see those messages start flying. Help me welcome Vital Ability, LLC as a partner.
Please take the time to make a comment, share your thoughts, and tell us what impacted you the most and what brought you here: Reviews and Testimonials
Your input is important to the development and growth of this website, and we like to know what is going on out there in your thoughts.
Thank you for visiting us! We look forward to hearing from you.
Phonomenal and groundbreaking news that had been spreading like wildfire there since May 2021 and then again in November 2021 – only to be met by disappointment and seemingly caught up in global financial politics and escaping what the focus should be: benefit of rehabilitation for the patients.
Essentially, what this means is that the SPECT scan is now medically recognized for the diagnosis and prognosis of traumatic brain injury (TBI). The SPECT test shows in much clearer detail the presence and extent of the brain injury (especially mild TBI), something that MRIs and CT scans cannot. See this article
Then the Ontario Superior Court of Justice released an important decision in Meade v. Hussein, 2021 ONSC 7850 regarding the use of single-photon emission computed tomography scans (“SPECT scans”). Justice Bale found that SPECT scans failed to meet the reliability foundation test for novel scientific evidence. See this article
This is of global interest and has the potential of benefiting millions of people affected with brain injury. It was noted that the the Canadian Association of Nuclear Medicine (CANM) unanimously adopted new procedure guidelines for brain single photon emission computed tomography (SPECT) imaging for psychiatry and neurology. The prestigious scientific body endorsed brain SPECT imaging for the assessment of many common issues affecting tens of millions of people. See this article
This is surely going to be a very hot topic where the medical community is finally catching up with technology and years of research. Sure to be on the forefront and not going away any time soon is the focus of getting our laws to also catch up with medical and technological discoveries.
This would also involve getting the Insurance industries on board to provide coverage for this diagnostic necessity and to provide better rehabilitative care to our survivors of brain injury and those suffering with mental illness.
I can speak from personal experience about my SPECT experience. It was a game changer for me. It validated all of my symptoms. It helped me not feel crazy, but allowed me to know just what to focus on as part of my rehabilitation process.
Having “proof” for something you know is true, because you are living it, is an overwhelming relief and was a hugely emotional process for sure. I was determined to get answers, one way or the other. This process helped me to be able to then focus on what I needed to improve and work on, to let the healing commence, and be able to move on to acceptance in the grief and transformation process of re-inventing myself. The results of the SPECT allowed me to be able to talk about my injuries in a more educated and informed manner.
I honestly wish I had been able to access the services from day 1 of my injuries. It would no doubt improved and perhaps even shortened the rehabilitation process. I am a staunch supporter of the SPECT scan and am hoping that there are ongoing landmark and groundbreaking determinations that benefit the quality of life of all patients.
Share this Blog with others. Share with a friend, a healthcare provider, a family member, a colleague, in a meeting, in an email, in a Facebook post, in a presentation, on other social media sites, on your own blog, etc. The possibilities are endless.
BENEFITS OF FOLLOWING the HOPE TBI BLOG:
Ability to read our latest Blog posts
Get email updates about added pages to the HOPE TBI website
Come and listen this coming Wednesday 8/10/2022 at 10pm EST as Kim and Co-Host Caren, will be discussing Navigating Mental Health after a Brain Injury, and reframing our thought patterns.
Can a brain injury lead to mental health conditions? How can we help ourselves self-regulate?
Check out the Orginal HOPEster. The Survival Story of our HOPE TBI founder.
It’s been a while since I have shared my story and I wanted to share it with those of you who may not know it. Thank you for being here as part of my ongoing recovery. I just wonder if we just continue in our process for the duration of our entire lives.
Isn’t the brain and the body magnificent?
“My name is Caren Robinson. I have always been a busy gal. Adrenaline junkie to some regards. Loved riding motorcycles, roller coasters, diving off bridges to go swimming, and also anything to do with The Arts really. I have always had a job since I was … Continue reading HERE….”
My Story page has gotten a wee bit of a face lift, and a few more clarification and more information added. Funny how as time passes, things are easier to talk about. At least some things.
Help us welcome our newest HOPEster. Cathy is from Everett, Washington.
“I got in a very bad car accident on August 8, 1976 when I was 14 and preparing to go to high school. I was born in the 60’s (1962 to be exact). That was a time when not a lot was known about the after affects of sustaining a severe head injury……..”
“…..If I could share any one message with all of you out there in the world, it would be to not give up. It’s never too late to get help, and keep fighting to get where you want to be in life, even if you have to do it a little bit differently than others.”
One of the biggest challenges is finding new hires who have disabilities. It’s difficult because they might not have the opportunity to work in a job where their disability is accommodated. For example, someone with hearing difficulties might be limited to jobs that can easily be vocalized.
If you want to attract differently-abled employees, you’ll need to put structures in place to accommodate those disabilities. In this guide, HOPE TBIshares some key tips for making your workplace more inviting to more diverse people.
Ideas to Attract Differently-Abled Applicants
SHRM suggests creating a more inclusive culture, making sure your website can work with assistive devices, offering career planning opportunities, and more. Reasonable accommodations are also important for different types of disabilities, such as allowing for part-time work, providing accessible transportation options, or any other type of accommodation that would help support your differently-abled employees.
Incentives for Differently-Abled New Hires
You should also think about what incentives you can provide for people with disabilities. For example, what if you offer an internship program for people with disabilities and then hire them once they graduate from the program?
It’s a win-win situation because you are able to reach out to this target audience and offer them the opportunity for advancement while providing valuable experience and skills training at the same time. Offering career planning opportunities can also help attract differently-abled new hires. It’s important that they have opportunities to think about their long-term plans in order to feel confident and empowered in any role they pursue.
Revamp Your Recruitment Process
When it comes to recruitment, make sure you’re including all different methods of sourcing and hiring. Keep in mind that people with disabilities are a viable pool of talent to consider when you’re looking for new hires.
For instance, IMPACT notes that you can make your website more accessible to those who need different types of assistive devices by making sure everything is in plain English and using contrast colors for text. You can also offer opportunities at your company for internships or mentorships for those with disabilities.
Finally, think about how your process may be excluding this group from applying. Maybe you don’t have an option on the application form for people who have certain types of disabilities? In order to find out where this might be happening, provide contact information on the application form so that people can ask questions.
Create a Budget for Reasonable Accommodations
If you’re interested in being an employer of differently-abled individuals, budget for reasonable accommodations in the workplace. This includes office supplies and furniture that can be maneuvered to suit those who have physical disabilities. For example, consider providing a desk chair with wheels so that an employee who uses a wheelchair can roll from place to place instead of having to walk around the entire office.
Other accommodations may include louder alarms or bigger signs because some people with hearing impairments or dyslexia may not hear or read things correctly. Budgeting for these adjustments will help you attract more diverse talent to your company.
In addition, a critical housekeeping step is to establish yourself with the state to make sure you are compliant with tax laws. This is also essential in yourEIN application, which is necessary for the IRS to use in payroll taxes and if you offer retirement plans.
Finding Differently-Abled Applicants
Michigan has several programs designed to provide disabled population services, as well as other related services. This is a good place to start if you want to connect with differently-abled people who are looking for employment.
HOPE TBI helps take the struggle out of finding resources and information when someone is faced with a trauma from a polytrauma or brain injury, and the resulting conditions from those injuries (acute or chronic pain, symptoms, experiences, processes, etc.) and various treatment options available. Connect with us today to find out more! hopetbi4ever@gmail.com
Did you learn something, read anything that inspired you or impacted you on the HOPE TBI site at https://hopetbi.com/ ?
HOPE TBI brings awareness, educates about self-advocacy, and helps take some of the struggle out of finding resources and information when someone is faced with a trauma from a polytrauma or brain injury, and the resulting conditions from those injuries (acute or chronic pain, symptoms, experiences, processes, etc.), and treatment options available.
Do you support bringing awareness to the topics written about and want to see more content? Check out our Blog at https://hopetbi.com/blog-and-updates/
Keep HOPE TBI active, growing and it services FREE.
You can support general operations, outreach, and awareness efforts of HOPE TBI by being a donor or sponsor at https://hopetbi.com/donations/.
(all yearly donators of $500 or more have the option to have their name, “in memory of” name, or business name/logo listed on our “Sponsors” page for one year after donation made)
Please take the time to make a comment, share your thoughts, and tell us what impacted you the most and what brought you here: Reviews and Testimonials
Your input is important to the development and growth of this website, and we like to know what is going on out there in your thoughts.
Thank you for visiting us! We look forward to hearing from you.
FAITH is stepping on the “seeming void” and finding the rock beneath.
With FAITH comes HOPE.
Where there is HOPE there is FAITH.
Where there is FAITH.
MIRACLES happen.
I can say with pure conviction that I would not have survived all that I have this far into my life without a strong connection to my Faith and my deep Spiritual Connection. I can say that throughout this recovery process, there are times when it feels that all I have that is consistent is my Spiritual self and my every present, life clinging grasp onto HOPE.
I am not without humility when it comes to the fragility of life in general. I am truly in awe of the miraculous events, too numerous to be coincidental, involving the wreck I was in and all of the circumstances in my life since. There were angel wings wrapped around my son that day. It is the only explanation for his survival….the only explanation for my survival. My continued courage to overcome seemingly insurmountable difficulties, medical and otherwise have only been conceivable due to my connection to God and the abiding Faith that I embrace. This propels me and gives me strength to never give up HOPE.
“Can’t” is not in my vocabulary as a general rule. I have never been that type of person to accept “can’t” as an acceptable answer. I feel this limits the education and growth of ourselves as individuals, professionals, spouses, family, parents, and friends. If at all possible, rid this word from your life. Instead replace it with “can attempt” “can make effort to” “can do it” “can accomplish” “can change my thinking about” and any other word or phrase that includes your ability to put forth the effort in living the opposite of “can’t”.
One of my favorite verses is Phillipians 4:13 “I can do all things through Christ which strengthens me”. This has fueled me for years.
I lived through this wreck for a reason. I was meant to survive. There is a plan, a special plan for my life. My life matters. I truly believe this. I am not here to merely exist without offering some meaningful contribution to my family and the world. I have been led to serve others my whole life. I have enjoyed this life of service immensely. I am grateful for the blessing that I have been given to continue my life’s journey. Sometimes, I am not sure why I was CHOSEN to live, while others with far less injuries have died – but I will not waste this time. It is precious, and every moment counts!
My dad used to say that many are “LED” but few are “CHOSEN”. I never understood that very much as a child, however, I feel I am getting a better grasp on this as an adult – especially as one who continues to survive from a Catastrophic and Life changing event (but then aren’t all life events life changing?)
I find myself led to continue to write about, speak about, and educate about my Trauma, my Survival, my Rehabilitation, and Self-Advocacy – so that others may perhaps find something useful from my experiences and I have a written expression of healing. I am enormously grateful to my mother for starting a blog for me in the beginning, and for being a testament for my life. The timeline of events that she has written about has been very helpful to me as well and helped me fill in a lot of blanks for things I just do not remember. I love seeing her posts and hearing her words like a warm blanket of protection. How she knows how to say just the right things still amazes me. I hope, in the end, that my kids love me as much as I love her; as much as she has helped me to continue to love myself. She is amazing.
I am blessed with a selfless and loving husband as well. He has sacrificed much for me. He makes me feel beautiful and shines light in my life, even in the darkest of nights. Not only did God Choose me, but so did he. My love for him is unyielding and he is simply the best man I have ever known in my entire life (before and now). He is beyond amazing and I am truly fortunate to know such love.
My HOPE is that I continue to evolve professionally and personally. My HOPE is to continue to be led to the proper medical care, and interventions to help me further my life as a functional, active, evolving, spiritual and passionate human being. My HOPE is that my family is continually blessed with support and strength to endeavor this journey with me. It has not been easy on them either.
I realize I will never be the same Caren I was before the wreck. That much is abundantly clear. The “new normal” I embrace I am still getting to know…….even years later. From being bent and literally broken, to a process of healing that incorporated plates, screws, nails, modern day technology and a sheer will to survive. I have been able to find value in the life I have been gifted to live. I am not perfect, I am far from it. There are struggles that still challenge the fabric of my existence. There are challenges and fears I still face. Sometimes, on a daily basis. However, I am grateful for the opportunity to face them and continue becoming the best version of myself possible.
We are allowed to be a masterpiece and a work in progress. I am a work in progress, my life is my masterpiece, and I am not giving up on ME. Your life, your story, your experience, your sheer grit to survive is your masterpiece. I see you. You are not invisible. Don’t give up on you.
If you are reading this, thank you for being here at this moment. Please don’t give up on me either. With your help, your ongoing support, your presence, your intercession, your skills, your energy – real or virtual, all things are possible.
Easter actually began as a pagan festival celebrating spring in the Northern Hemisphere, long before the advent of Christianity. “Since pre-historic times, people have celebrated the equinoxes and the solstices as sacred times,” Later, Easter became recognized as the highest celebration of Christianity. Because the resurrection establishes the belief in life after death. Happy Easter if that’s you. However you believe, spring signals a time of renewal, when new life and color emerges.
Add the Virus and other news hot topics the past few years, and there has been ample opportunity for us to have reason to grieve. With more isolation, lock downs, fear mongering .. Grief over real losses of all kinds, has perhaps been even harder to bear. Grief is stressful enough, but add everything else mentioned, and no one has been immune to grief. We must take time to grieve, or we would never fully appreciate gratitude.
Tonight we discuss grief and renewal for brain injury survivors. We’ve felt the sorrow, now how do we refresh and move forward?
This show is a gathering place for anyone seeking recovery from the challenges of life on life’s terms. We discuss useful tools that have helped us lighten the load, of our journey through recovery. This is a “we” recovery program, because it is in the “we,” that we find the new “me.”
We focus on the four A’s of Recovery: Awareness, Acceptance, Action and Adaptation. This is a place for survivor’s striving to become thrivers, which takes a good bit of Warrior!
Hosted by Kim Justus, author of In a Flash: Miracles Here and Beyond and Hootie’s Hollow and the Magic Tree found at inaflash.org and Amazon & “Like” me at facebook.com/inaflash.org too! For More on Caren’s great Blogs and Resources see: hopetbi.com
This is where it all began. The HOPE TBI Blog and the HOPE TBI Website.
It all began with my mom starting a blog and fundraiser on my behalf, years ago. My mom has been one of the many valuable supports in my life, through everything. She never gave up on me; for that I am grateful.
I asked her to collaborate with me to do a story page to honor her and the process she put so much effort into on my behalf. This is that story.
This is an excerpt from the Paper written by renowned Neurologist “Masel”:
“……The purpose of this paper is to encourage the classification of a TBI not as an event, not as the final outcome, but rather as the beginning of a disease process. The paper presents the scientific data supporting the fact that neither an acute TBI nor a chronic TBI is a static process—that a TBI impacts multiple organ systems, is disease causative and disease accelerative, and as such, should be paid for and managed on a par with other diseases. Despite the fact that patients with a TBI who survive the acute event do not die of their brain injury per se, a TBI is a disease…….”
Masel, B. Conceptualizing Brain Injury as a Chronic Disease. Vienna, VA: Brain Injury Association of America, 2009.
This is a post I wrote just as I was really learning to claim my role as an advocate for myself. It was a turning point for me, in truly learning to trust my body and not necessarily what I was told about my body. It was when I decided to trust MYSELF, and to speak up when I felt or knew something was wrong.
This experience with this nightmare provider was someone I should have been able to trust. It turns out he took advantage of that trust. This experience brought me to a painful realization that not all doctors respect the “do no harm” oath.
In fact, if left unchecked, those who don’t value that oath, can cause a great deal of additional irreparable harm to their patients, can absolutely cause medical PTSD, and change the course of a patients care for the worse. I share this again as it should not be forgotten.
Find your voice and speak up for yourself. You are worth it
(previously posted elsewhere in 2014, yet worth reposting)
The Golden Girls
Golden Girls Explain Golden Opportunities
TBI is an invisible disease….so is PTSD….and so are things that are obvious injuries if NOT actually checked…..if the doctors actually LISTENED to their patients and did the tests and procedures they were supposed to from the beginning rather than making judgements without following through – or without actually consulting the patient about their decisions.
This is essentially what happened to me too. I was in a vehicle accident with polytrauma and Traumatic Brain Injury and several fractures. Then I keep complaining all through therapy that my pain was worse and I was losing strength on my right side. I was released to attend PT OT and ST without restrictions that during and after therapy….I spoke of my pain and limitations often. Not the referring Orthopedic Dr. nor the Rehab Dr. ever did a CT Scan to follow up on my pain or x-rays of all the previous fractures. In fact, the Rehab Dr. said it was probably all anxiety related and I needed to put in “more effort”…He even held my arm up and dropped. I couldn’t hold it up on my own. He thought I should try harder – what he didn’t accept is that I was giving it all that I could. It just wouldn’t work….and now I know why. As it turns out for the last 9 months I finally get that CT scan and it shows that my ribs 2-11 are still fractured and displaced with NO HEALING…and that shattered and fractured scapula on the R side?….YEP….no healing either. I am now scheduled for surgery Oct. 8th to plate and put screws on each rib and reconstruct my scapula/body and plate and screw those as well…..obviously THEY weren’t putting in enough “effort”…. if they only listened to me. Feels good to be validated and know that I can actually trust my own judgement about my body though…my PCP on the other hand has been great so far….I have a medical case manager too who has been advocating for me as well….I can say that they only added to the anxiety I was already having about the wreck in general….those other doctors, that is.
This is a great episode from the Golden Girls show about Invisible Illnesses where she confronts the Dr. who didn’t listen to her…..this is just AMAZING!!!
I only wish I could do this with my Nightmare Doctor….
Compilation of all the doctors Dorothy went to and the process she went through to get answers:
Let us introduce you to Stephen Bristow. He is from Michigan and has a unique story of how the system sometimes fails it’s children. This story also drives home the importance of adequate services and interventions that are both compassionate, ongoing, and swift; a stark reminder of just how far we have come with the treatment of Brain Injury over the years, and how much further we have yet to go.
“I was young about five years old or younger when I sustained my first traumatic brain injury. This was caused by my father. He was very abusive. He was also a Navy man. The second traumatic brain injury I recall happening around 7 or 8 years old, and had something to do with baseball The one titled “mother” was not around most of the time. When she was, she was also abusive, and I sustained many beatings from her. She was employed at a Utility service…….”
The term “traumatic brain injury” wasn’t something I ever thought too much about pre-accident. It was something that happened to people in stories in the news, it was something that happened to people in the movies. It never occurred that it was something that could happen to me. And then it did. ----
This group is to list durable medical equipment, supplies, technology, machinery, prosthetics, etc. that you are ‘gifting” for FREE to someone in need.
You may also post a request if you are needing something as well. Please only request item(s) if unable to acquire by any other means. No acquiring items just to sell them.
THIS GROUP IS NOT OPEN TO VENDORS.
[Disclaimer: This group does not support or endorse the exchange of medications or supplements in any form. Please see your medical providers for those needs. This Group or its Owners/Moderators are not responsible for any transactions, equipment, or product exchanges with another member]
Gifted Items/Needed items can be, but are not limited to: vehicles, hospital beds, wheelchairs, braces, ventilator equipment, oxygen concentrators, traction equipment, personal care aids, books, Posey Lifts, adaptive equipment, Manuals/information, Bathing Supplies, mobility aids, etc – and other items useful to a person with a disability or injury. The sharing opportunities are endless.
We realize that Insurance does not always cover all the needs a person has after experiencing a devastating and catastrophic medical emergency. We also realize not everyone has insurance. We understand being financially strapped, destitute, or handicapped after a life changing medical event.
Being a member of this Group does not imply nor guarantee that you will have your needs met or provided, but merely an additional opportunity to network with those who may be able to help directly or indirectly.
This Group will also allow you the opportunity to share your fundraising pages or place to post your public funding request page links (like Go Fund Me Page, PostHope page, Pay It Forward Page, YouCaring page, Give Forward, Donors Choose, etc). Be prepared to be vetted for authenticity.
It is strongly advised that if you meet anyone offline, that you do so in a public and safe location.
We want to introduce a Survivor story and a Caregiver story. The battle for survival and quality of life continues with these two powerful stories.
Debbie Webb – “The year was 1990, I was practicing barrel racing and the horse I was riding slipped onto her side. Upon impact with the ground, I was immediately unconscious.” Check out her story here:
Kris Ruckle-Mahon – “My role went from being a parent to a caregiver on April 11, 2007, something I was not financially prepared for. I was fortunate though, to have a great work and family support system to help us through it.” Check out her story here:
Grab a cup of tea or coffee and snuggle in for a read of the Survivor story about Chasity Christian. A survivor of many traumas and how love is carried in different forms – from our newest HOPEster.
Hello HOPEsters. We are thrilled to be able to share with you a list we have tirelessly compiled of “clinically practicing” Neuroendocrinologists who provide direct patient care.
This is not an all inclusive list and does not include Neuroendocrinologists that are “researchers or lecturers” only.
Let us know of any others that are not on the list and we would be glad to add them.
Also check out our Neuroendocrinologypage as well, if you haven’t already done so.
Ya’ll have seen and heard me talk about Auto no-fault a lot over the years. You have heard how I have embraced self-advocacy on my own behalf and encouraging such with others as well.
Some changes were made to the Michigan Auto No-Fault laws that have hurt the protective measures that No-Fault owes its recipients. It has been disastrous and is literally costing lives.
Check out C-Pan (Coalition Protecting Auto No-fault) and Michigan Auto Law for more information and the various changes.
However, not all HOPE is lost just yet.
THOUGHTS?
Here’s an idea to bring awareness to Michigan No-Fault Laws/Changes, an invitation to all Senators, lawmakers, and our Governor to “Have A Heart”.
Each legislator who has voting power on the No-Fault issue, spend one week. Just one…..with a catastrophically injured patient and their family. They have to be a caregiver for that week, working with family or nurse supervising direct care..
Then let’s see how they think at the end. I think before pushing paper and making decisions from behind a desk that impacts so many lives….they should be required to live it in some way and make it work by their own effort and examine what they are expecting (56 hours limit being suggested for example) before making laws for it.
It’s easy to judge if you aren’t living it every moment of every day.
We could call it OPERATION: “Have A Heart”
#haveaheart #wecantwait
Here are suggested parameters:
Live with family in their home for 7 days. 24/7 (live there, sleep there, be available all 24 hours – regardless of activity involved in at the time)
Provide direct care to patient along with caregiver (regular or fill-incaregiver, or at direction of family)
No personal tablets, laptop computers, other electronic devices allowed to be brought into home. No use of phones during care time.
No refusing to do any care needed (due to discomfort, grossness, lack of knowledge, or fear of messing up).
No mistreatment, verbal abuse, or physical abuse of patient or family.
No help from anyone outside of what family has immediate access to without you there (no assistants, runners, interns, etc)
No buying or purchasing anything for yourself (including food or drinks) or the family until after 7 days are completed. They eat and drink what family does on their budget.
You may be asking yourself how you can help. How can you make an impact to continue to bring awareness and support self-advocacy? How can you become a HOPEster?
Maybe you don’t have a Brain Injury and have never experienced a Polytrauma. Maybe you came upon this Website while searching for something else. Perhaps you are curious about the content, or know someone who has had a Concussion, Brain Injury or a disability.
Whether you are here accidentally or purposefully we hope you have found information and resources in this Site that have been helpful, useful, or educational to you. If this page is your first stop – please explore the rest of our pages as we offer a lot of value for your visit. We provide all these services for FREE to the community at large.
Maybe you are a survivor, a caregiver, a healthcare provider who understands all to well the content here and could even add to the stories here with your own.
If you would like to offer HOPE (Help One Person Excel) by:
Giving a gift to keep this site running and helping its services remain FREE
Help us continue to bring awareness; or just support the cause
We are thrilled to announce another way of bringing support to you, and awareness to brain injury and polytrauma. We are pleased to introduce you to our Podcasts.
If you couldn’t get enough of the HOPE TBI website, Blog, or Support Groups… you are going to love listening to our Podcasts.
If you are someone that has difficulty reading, or is on the go and no time to peruse web pages, you are going to love the convenience of listening to our Podcasts.
If you are new to HOPE TBI, then welcome. We have a lot of support to offer you through our many FREE services.
Please remember to leave a Testimonial to give us feedback. Do you like what you hear? Are you getting value from the content? What impact has HOPE TBI made in your life. We want to know.
Check out the story about a mom fighting for the life and proper care of her daughter who was hit by a car January 2021.
When doctors and therapists don’t have faith, sometimes a family’s love and prayers can work miracles.
Michelle Patnesky, the mom of 17 year old Hailee, takes us on a journey with her family as they traverse the system to advocate for their daughter who has sustained a severe brain injury and remains in the hospital.
Check out our newest story submission. at HOPE TBI www.hopetbi.com
Vera Quijano, a dance and yoga Instructor, who is now dancing to the beat of a different drum after sustaining a Traumatic Brain Injury after surviving a vehicle accident, where she was hit by a drunk driver.
I just want to say to all you Mothers’s, Step-mothers, Foster Mom’s, and Guardians fulfilling a role as a “mother” figure…..
I see you.
I see your love, your sacrifice, your devotion, your fierce advocacy, your struggle, your effort, your laughter, your tears, your disappointment, your celebrations, your resentment, your anger, your amazement, your exhaustion, your selflessness, and your commitment.
I just want to say to all you Mother’s, Step-mothers, Foster Mom’s, and Guardians fulfilling a role as a “mother” figure….
I hear you.
I hear your cheers, your jeers, your concerns, your focused topics, your questions, your accolades, your encouragements, your motivational speeches, your yelling, your frustration, your grief, your joy, your coaching, your mediation, your compassion, and your ongoing effort at communication.
I just want to say to all you Mother’s, Step-mothers, Foster Mom’s, and Guardians fulfilling a role as a “mother” figure….
Just Be You.
Be the best version of yourself each day, be that disheveled mess, be that organized detailed version of yourself, be true to your values, be that parent that can admit their mistakes, be that parent that lives by example, be a stay at home parent, be a working parent, be a disabled parent, be a retired parent, be scattered, be focused, be hard to understand, be easy to get along with, be the parent that lacks humor, or be the parent that can make your child laugh. Just be YOU.
You are who your child(ren) will remember long after they have grown and you are their influencers for good or evil, love or hate, bravery or fear, joy or sadness, loved or abandoned, condemned or celebrated. You are the beginning of their imprint on the world.
Thank you for being just who you are and adding to the fabric of our world with your ability to be THAT MOTHER.
Brain Injury Awareness Month Join the #MoreThanMyBrainInjury Campaign this March
The Brain Injury Association of America (BIAA) leads the nation in observing Brain Injury Awareness Month by conducting an awareness campaign in March each year.
The Brain Injury Association of America (BIAA) theme for the 2021 to 2023 campaign is More Than My Brain Injury.
Kim and Caren discussed, reaching out and staying connected during this difficult time in our history. We discussed tips and ways to stay connected.
We took callers .. Interested in hearing how our listeners are coping with the “New World” and their thoughts, fears, feelings.
This show is a gathering place for anyone seeking recovery from the challenges of life on life’s terms. We discuss useful tools that have helped us lighten the load, of our journey through recovery. This is a “we” recovery program, because it is in the “we,” that we find the new “me.”
We focus on the four A’s of Recovery: Awareness, Acceptance, Action and Adaptation. This is a place for survivor’s striving to become thrivers, which takes a large dose of Warrior!
Hosted by Kim Justus, author of In a Flash: Miracles Here and Beyond found at inaflash.org & “Like” at facebook.com/inaflash.org Co-Host is Caren Robinson found at: hopetbi.com
I wanted to reach out and share our latest and greatest page with all of you. It is our Reviews and Testimonials page.
If you are seeing this message in your email you have subscribed to our email notification list. That means you care enough about our content to want to be notified when we post something new.
If you are coming on this Blog post by scanning our Site, please take time to also leave your review and feedback after exploring a bit.
We would be thrilled and grateful if you would take a few moments to type up a review or feedback about our website and submit it in the comment section of our new page.
Okay….as an advocate for patients with brain injuries and those going through transitions in their life….part of that advocacy and role of consulting is being authentic and realistic as well. While I have compassion for what Biden is going through health-wise….I also must be pragmatic and realistic about what we as a Country are watching and a lot of America is missing.
We are watching in Biden a man struggling with brain changes that make him inept for the role of President of the United States. He is losing time, memory, has numerous bouts of aphasia and an obvious onset of what appears to be dementia. While he may go on to live many more years and contribute to society in other ways……the decline is palpable and not representative of what our Country needs or requires of a Commander -in-Chief.
Biden is NOT someone that should be in a role that requires strong mental faculties to run this Country…..he absolutely can not win against Trump or any other Republican candidate for that matter.
Bernie is our only hope at this point to have a fair, constructive, and challenging election in November. It won’t be a challenge if the DNC foolishly allows Biden to continue on. Biden will lose and should lose as he is just as dangerous for our Country as is Trump.
I hope Bernie pulls out a win to face off against Trump. I hope there is not a Baker convention that picks someone less qualified or not even in the running…as the Superdelegates would surely do….
We are facing a historical and pivotal shift in our Country and have been for quite sone time I only hope it shifts in the way that saves our Country and its democracy….not destroys it.
Come and Listen to our recorded Radio Show called Recovery Now with Kim Justus and Caren Robinson as we talk about Love, Sex, and TBI – Beyond the Chocolates.
We would love your feedback. Feel free to share the link and start a dialogue.
Sexuality is one of the most complex aspects of life but, the sexual lives of people with disabilities have been disregarded and stigmatized. As a result, sexuality as a form of pleasure and an expression of love is not taken into account or even recognized for individuals with disabilities.
Sexual expression is influenced by cognitive and emotional processes and is dependent on functioning anatomical and physiological systems, in other words, our brains control our sexual organs and responses.
Before resuming sex with a partner, boyfriend, girlfriend or spouse, talk about it with your doctor or therapist and be guided by their advice. Make sure you are clear and talk with your mate about your expectations, fears and feelings, including consent. Communication is key! Remember to not put too much pressure on yourself, focus on pleasure and not technique. You may need to change your same old lovemaking style and experiment with other sexual activities which can include
oral sex and mutual masturbation
utilization of sexual aids/toys/furniture
to increase intimacy, concentrate on boosting the romance in your relationship by offering lots of affection, complementing and saying nice things to each other and celebrating big and small occasions.
Importance of safe sex
After a TBI, it is just as important for you to protect yourself from unplanned pregnancy and from sexually transmitted disease as it was before your injury. Even if a woman’s period has not returned, she can still get pregnant. Here are some tips to help with birth control and protection from sexually transmitted disease.
Do research to help figure out what method of birth control and protection from sexually transmitted disease are best for you.
Because of changes in thinking abilities, it may be harder for you to remember to use protection or to remember to take it with you.
You can plan ahead by always carrying a condom or other method of protecting yourself and your partner.
For women who use birth control pills, or a device that must be replaced, using a calendar or alarm on a smart phone can help you remember to take the pills or change the device.
If you are unsure whether your partner has a sexually transmitted disease or has been intimate with others who have such disease, it is safest to use a condom.
If you have engaged in any risky sexual behavior, one of the best things you can do for yourself is to get tested for sexually transmitted diseases and get treated if you test positive.
Consent should not be assumed
Each of us is responsible for making sure we have consent in every sexual situation. If you are unsure, it is important to clarify what your partner feels about the sexual situation before initiating or continuing the sexual activity. Consent should not simply be assumed by:
Body language, Appearance, or Non-Verbal Communication: One should never assume by the way a person dresses, smiles, looks or acts, that they to have sex with you.
Dating relationships or previous sexual activity: Simply because two or more people are dating or have had sex in the past does not mean that they are consenting to have sex with you.
Marriage: Even in marriage, a person should not assume they have consent for sexual activity. Marital rape is as serious as any other sexual assault.
Previous Activity: Consent to engage in one sexual activity at one time is not consent to engage in a different sexual activity or to engage in the same sexual activity on a later occasion.
Silence, Passivity, Lack of Resistance, or immobility: A person’s silence should not be considered consent. A person who does not respond to attempts to engage in sexual activity, even if they do not verbally say no or resist physically, is not clearly agreeing to sexual activity.
Incapacitation: Alcohol consumption or use of other drugs can render a person incapable of giving consent. Alcohol is often used as a weapon to target individuals and is used by perpetrators to excuse their own actions. Additionally, Michigan Criminal Sexual Conduct laws apply to a perpetrator regardless of whether or not they were drinking. It is important to remember that sexual assault is never the survivor’s fault, regardless of whether they may have been intoxicated.
The term “sexual assault” means any unwanted, nonconsensual sexual contact of any kind (including kissing) obtained through the use of force, threat of
force, intimidation, or coercion.
Rape is unwanted, non-consensual sexual contact that includes penetration (i.e. vaginal or anal penetration, oral sex, and genital touching) obtained through the use of force, threat of force, intimidation, or coercion. 18% of all rapes and sexual assaults are reported to be committed by strangers, which means that most of these crimes are committed by someone the victim knows, is close with or related to (according to the 2017 Bureau of Justice’s).
Myths About Disability and Sex
Disabled people can’t have sex.
Disabled people have to pay for sex.
Disabled people aren’t sexy.
Disabled people don’t want or need sex
Disabled people only have kinky sex
Disabled people can’t have sex
Disabled people only have sex with other disabled people
Disabled people can’t have kids
Disabled people shouldn’t have kids because they can pass on their disability
If you have sex with a disabled person you will catch what they’ve got
Disabled people are a burden on their partners
People living with a disability can’t have “real” sex
Disabled people need protection, like kids
Disabled people have more important things than sex to worry about
Disabled people are brave and courageous to try sex (no, it’s just adapting to a lifestyle)
All persons in wheelchairs are chronically ill, frail, or sickly
Facts About Disability and Sex
People with disabilities can be sexual and enjoy sex
Some people who use a wheelchair can still feel “down there”
Sex is not just all about each others “privates”, it’s about intimacy as well
Mobility aids can be a fun addition
People with a physical disability don’t just “lie there”
Disabled people can have sex and enjoy it
Disabled people sometimes choose to pay for sex like people who aren’t disabled
Disabled people are sexy
Disabled people can have sexual desires/needs
Disabled people can have kids and build families of their own
People with disabilities can identify as LGBTQ too
It can be very frustrating if your life is being negatively impacted by your memory loss and someone (often a friend, provider, or relative) who doesn’t truly understand your experience says, “Oh, I forget things too…”
You may hear some people say that everyone has memory loss, especially as we get older. To some extent that is a true statement. We all have moments where we walk into a room and forget what we walked in there for, or forget where we laid the keys down at. However, here is where it differs. Memory loss as a result of a disease process, injury, or due to the use of certain medications is different than the memory loss we experience as part of the natural aging experience.
Several conditions, other than aging can cause significant memory loss. Some of these may be reversible with treatment. Some are permanent, even after treatment. Regardless of whether reversible or permanent, if it is effecting your life in a negative way, or robbing your quality of life, you may find some of the tips below to be helpful in helping you manage the memory loss you or a loved one may be experiencing
Some examples of memory loss that are not included in the natural aging process are the following:
Brain injuries – traumatic or acquired (such as blunt force trauma, accident, encephalopathy, falls, blood clots, stroke, transient ischemic attack, aneurysm, medications, drugs, etc)
Result of brain surgery (all surgeries carry risk, especially surgeries involving the brain – examples may include shunts, removal of diseased tissue or tumors, repairing bleeds, repairing puncture or crushed wounds, etc)
Brain Diseases (like a tumor, hydrocephalus – fluid in brain, or other rare disorders) and other Diseases (like Huntington’s, Muscular Dystrophy, Parkinson’s Disease)
Infections of the brain – such as syphillis, HIV/AIDS, Lyme Disease, other viruses
Vitamin B1 or B12 deficiency – good nutrition is imperative for brain health
Hypothyroidism ( a common secondary condition that can be acquired after head injury and often undertreated; some can be hereditary and if left untreated can exacerbate symptoms)
Kidney or Liver disorders
Dementia/Alzheimer’s (may be acquired secondary to brain injury, inherited, or from other unknown processes)
Emotional Disorders – stress, anxiety or depression can cause forgetfulness, confusion, difficulty concentrating and other problems that interrupt the ability to function in daily life)
Alcoholism, smoking, or drug use
Sleep Deprivation – quantity and quality of sleep affect our memory processing
Here are 12 ways that may help you manage your memory loss in a more functional way, helping to maintain as much dignity and independence as possible.
Make a memory board (with important names and frequently used phone numbers). Hang somewhere visible, so it can be seen and utilized daily. Update the same day weekly or as schedules change.
Create a life story book, photo album or something digital that is labeled to help identify who and what is important to remember (people, places, experiences). Get assistance to from someone you trust (such as a family member or professional) to do this. This can include pictures, question and answer format, or whatever works for your particular needs. This serves as a dual purpose as well, as it can also be used by professionals or caregivers to understand more about you as well.
Cognitive stimulation. This involves activities and exercises that stimulate thinking, concentration, communication and memory. Utilizing brain exercise sites such as Lumosity , Constant Therapy, and CogniFit Brain Training; play strategy games (like cards, checkers, chess, crossword puzzles, word finds, puzzles); coloring, drawing, or listening to different types of music.
Utilize a reminder system (this may include calendar, white boards, chart on the wall). It could be color coded as well (so a different color for each person or different color for each appointment on schedule – just make sure you use same color each time you do the schedule). Using A Planner or a Calendar App? – write down things right away – without exception. Always keep the planner with you wherever you go. If you get a call about an appointment, write it down IN THE PLANNER. If something changes in the schedule, write it down IN THE PLANNER. Label cupboards and storage containers as a reminder of where things are kept; label doors as a reminder of which room is which.
LISTS are your friends and great reminders (note: if you have trouble writing, use a voice recorder or dictaphone to make lists). Consider making permanent signs – even having them laminated, to remind you of things you need to do regularly (for example – sign by the sink reminding you to wash your hands before cooking or before leaving the bathroom). Make a list for things you are running out of and leave attached to the refrigerator door (this is a great way to make a grocery list you take to the store with you). Make a list of what bills are due on what days and how much each bill is that is due, along with how it is paid. Make a list of daily tasks that need accomplished. Make (or have someone make) a checklist to hang by the front door that includes what you need when you leave (for example: purse/wallet, phone, phone charger, planner, meds, bottle of water, keys, sunglasses, ear plugs, jacket, etc). Use the checklist EVERY TIME before you walk out the door. This reduces chances of forgetting things.
Use post-it/sticky notes. You can use them anywhere in your home or personal workspace to remind you to do specific tasks (such as a sticky on a library book that has to be returned by a certain date, or start load of laundry today, etc).Once you have completed the task, it’s important to throw the post-it/sticky note away. This way you won’t accidentally redo what you already finished.
Use a mobile smartphone (cell phone). Many mobile phones have a built-in voice recorder. Use this to record information that you need to remember or add items to your virtual calendar. You could also leave recorded notes, play it back later, or review those notes at the same time each day. Also cell phones are great resources for text reminders, checking emails, and having access to a GPS (such as Google maps) to utilize to keep from getting lost. Use your phone to take picture of your whiteboard schedule that week so when you leave home you can look at the picture even if you aren’t at home to see it. Use an app to record incoming/outgoing phone calls (check your State or Country laws first though, about recording these in your particular location).
Medicine/Pill reminder box. This will help you see whether you have taken your medications for that day (this helps to prevent taking your medications more than once). Some models have am/pm, and other times of the day; some can be set to remind you when to take your pills, with an alarm, vibration or flashing light.
Use an alarm clock, a watch with an alarm, or a kitchen timer to remind you when you need to leave the house for an appointment, or when you have to check something cooking in the oven. Write down why you have set the alarm – so you know why it is going off. (I cannot tell you the number of times I have had an alarm going off and then sat there wondering why I set it. So notes are very helpful – put by the alarm)
Never leave the room when you are cooking. You may forget what you were doing and this increases risk of burning your food, burning up a pan, or causing a fire. Never leave the room when water is running in a sink or bathtub. You may forget about it and cause a flood.
Appointments and Meetings. In advance, make a detailed list of what you want to say, questions you have, agenda for meeting, etc. If you are going to a medical appointment, bring a pre-typed list to leave with the provider of all other providers/specialists (make sure this includes their addresses, phone numbers or contact information), all medications and their dosages (remember to list any herbs, supplements taking), and list of concerns. Record meetings or appointments to go back and listen to later and take notes from the recording.
Don’t procrastinate. Whenever possible, doing things when they’re on your mind rather than later so you don’t have to worry about forgetting them. Try to utilize the same routine every day as much as possible. Routine reduces chances of forgetting.
Open Letter to the President of the United States of America.
1/24/2020
Dear Mr. President,
Your role as a leader of the free world is the most important in the Republic, in ours….these United States and all her territories. Your role affords you the ability to maintain influence, direction, opinions, and historical precedence through each of your spoken words, deeds, and continued representation of various topics.
While I understand you are not a medical professional, nor have received any form of medical training Mr. President…you only need do a simple internet search on an internet browser of your choosing…. to read about the extensive life changing effects of Traumatic Brain Injury.
These medical facts are documented by a multitude of research/studies, medical professionals/experts, well respected organizations, survivors, and our very own Military.
Please understand, how recently, you painted an illustrative picture to the world about your seemingly misguided and uninformed statement about the lack of seriousness brain injuries cause.
Mr. President the potential life changing affects of Brain Injuries (also called Concussions by those not aware of the proper updated terminology) are VERY SERIOUS.
I was listening to your statements of ……..
[Mr. President] “No, I heard that they had headaches, and a couple of other things, but I would say, and I can report, it’s not very serious,”
[Mr. President] “They told me about it numerous days later, you’d have to ask Department of Defense, “I don’t consider them very serious injuries relative to other injuries that I’ve seen.”
“I’ve seen what Iran has done with their roadside bombs to our troops. I’ve seen people with no legs and with no arms. I’ve seen people that were horribly, horribly injured in that area, that war,” Trump said.
“No, I do not consider that to be bad injuries, no,”
Mr. President, I feel it imperative to provide you with the proper information on the campaign to bring global awareness to the effects of Brain Injuries. Awareness that even the White House seems to be in much need of….. so as to represent the dire importance of presenting the consequences accurately to the masses.
The effects of Brain Injuries can be long lasting or even permanent. While recovery and rehabilitation are possible, most people with brain injuries will face life challenges that will require them to adapt and adjust to a new reality where permanent physical or mental disability, and sometimes even death are the very real SERIOUS EFFECTS of their lives after sustaining that injury (or series of injuries). Even patients who appear to fully recover after treatment and rehabilitation may have some long-term symptoms that never go away or fully resolve. These changes may cause an inability to return to their life in the same capacity that they had before their injury.
Indeed Mr. President, injuries to the body, whether visible or not visible, can be equally life changing.
The statement you gave was partially correct in as one of the many symptoms of brain injury does include “headache”…..however there is so much more.
SOME of the other changes other than headaches include an alteration in:
an alteration in cognitive processes ( memory issues, distractability, impulsiveness, mood disorders, language, mental processing time, confusion, etc);
an alteration of senses (sight, vision, phtophobia, double vision, smell, taste, hearing, tinnitus (ringing in ears): aphasia (difficulty with talking or expressing ideas, understanding everyday language, and problems with reading and writing),
and development of PTS (post traumatic stress) and PTSD (post traumatic stress disorder) can also be present along with, or secondary to, the brain inury or polytrauma event(s).
[not an exhaustive list by any means]
Mr. President, despite the amazing advances in medicine, research by scientists, and active steps taken to develop treatment plans by our own Military; there are still more discoveries to be made and more work to be done.
Devotion of time and much needed funds, resources, and bipartisan support is still necessary to bring awareness and education about brain injuries to the forefront by not only you, but our other Leaders in our Government, private, and public sectors .
We must recognize this as a valuable opportunity to address this as what it actually is….a call to action about this – an International medical crisis.
We must figure out how best to treat those with Brain injuries, help them live their best lives, and be open to various methodologies and alternative sources of therapies that are allowed and covered by our insurance companies as to support the best outcomes.
Mr. President, you must know as soon as possible that despite early diagnosis and treatment of Brain Injuries, the fact remains that brain injury will be a life-changing experience for many patients.
So….in a word Sir….S E R I O U S !
HOPE for Life, Caren Robinson – United States Citizen Polytrauma and Brain Injury Survivor
I had the opportunity to co-host an online radio show LIVE.
We discussed “The Cost of Trauma on Recovery Now”. We were covering the cost Social Trauma vs Individual Trauma and shared a dialogue about our views and defining of terms regarding Trauma.
Something we didn’t have an opportunity to cover is the generational movement of folks not wanting to have kids at all or build their own families due to the potential exposure to Trauma, violence, or the eroding of society, our humanity, and the environment as a whole and how the current Trauma’s and experiences in our societies are impacting the future of humanity. It is imperative that as a collective consciousness we develop and implement ways to reduce, recover , and or eradicate as much Trauma as possible.
Please take an opportunity to share the link with those you feel will benefit from this topic.
Feel free to click on the link yourself as well and listen to the show.
Well I did something magnanimous this past Wednesday evening. I had received an invitation to be interviewed on Brain Injury Radio by Kim Justus.
I took the plunge, and embraced the opportunity to share some of my experiences over the course of the last 5 years in regards to bringing awareness to Polytrauma and Traumatic Brain Injury on a International Radio Show. How exciting to be a part of something so deeply personal, meaningful, and far reaching.
Check it out…take a listen and leave a comment below. Let me know if there was anything on there you could relate to. Feel free to share this link with anyone you think would benefit from hearing its content. I’d love to get your feedback!!!
Some of the resources mentioned on the show were the following:
Audiology testing, SpectCT Scan, Medical Acupuncture, alternative Medicine, cognitive fatigue (neurofatigue), among other things….and the mentioning of the following groups:
Being a mother has been the best job in the world to me. I always wanted to be a mother…from a very young age. I felt capable, ready, and committed to being the best mom possible. I wanted to be, and often was, the supermom, who could seemingly do a little bit of everything at a moment’s notice. Then the wreck I was in changed all of that forever. It shook my confidence. It shook how I existed from one breath to the next; it shook every aspect of my life as a daughter, sister, wife and as a mother.
I have been a mother to foster children, stepchildren and biological children. I have been a mother figure to kids that never even lived with me. I have been mothering to kids I came into contact with. I am convinced that how we care for, love, and embrace our children is exactly what makes us a mother, no matter how those children came into our lives, or became our own.
After the polytrauma and traumatic brain injury, I was no longer the mother my children knew before that day. I was different. I didn’t even know who I was. I was injured, I was in pain and I was unavailable emotionally, mentally, and physically. I have heard stories about things I don’t remember – things I have allegedly said or done, most humorous, some horrible and embarrassing. I apparently was a horrible person sometimes, especially in the first year after the wreck. This was just bad mojo – cognitive changes, personality changes, and enormous pain from all my injuries. I was often in so much pain I couldn’t function at all. I was useless to everyone around me. I definitely couldn’t make effective and meaningful decisions. I couldn’t remember one day to the next or who had visited me, or what was said by whom. I couldn’t muster taking care of anyone else, let alone myself.
My outlook on everything, while hopeful, was also littered with confusion and a myriad of emotions I didn’t seem to be able to control. I noticed my mood was worse as the pain increased and for a long time just breathing or moving caused me pain. I slept A LOT. I couldn’t even force myself to stay awake. I wasn’t the mother I had always been. I was the mother fighting for life and fighting to come back to my family. I was a mother still inside, still to my children, still to the world who knew me as their mother. Yet I wasn’t at the same time.
My own mother took care of me. She bathed me, clothed me, fed me. My mother was there for my first steps as an infant and again as an adult as I learned to walk all over again. My mother was my caregiver. She didn’t have time to grieve. She became the needed mother role for my children. My husband and my mom were my pillars of care and support. I was fortunate to have such amazing support. Not everyone has a supportive system like that. Some days my mom was more of a mother to her grandchildren for a period of time than I was….than I was capable of being. I don’t like to dwell on that. I don’t like that this was her reality – however I am enormously grateful.
I realize that being a mother is an enormously different experience for every woman who ventures down that path, and the experience is different with each of our children as well. I am acutely aware of this. Not every woman wants or enjoys being a mother. Some mothers are not mothering at all. Some women abuse or neglect their children. Some women wish they never had children. Some are the opposite however and actively involved, readily available, completely vested, and doting.
My job as a mother is constant. Being a mother is a full time endeavor and is totally consuming, no matter how old your children are, or how many you have. No matter how old, how broken, or how healed you are as that mother. A mother sometimes worries for her children. A good mother desires to see her children succeed. It is frustrating and depressing when you go from full time, full speed ahead in parenting and life to an abrupt halt due to an injury that doesn’t even allow you to participate part time…if at all on some days.
Learning to embrace the new normal after catastrophic injuries is no easy feat. Most days it seemed impossible and almost always overwhelming. You would be amazed at how much the love of being a mother motivated me to give my best effort each day. Some days, literally the only reason I found myself able to face the day was because I knew my children needed me, were counting on me, and were hoping for my recovery. So in that regard, the kids helped save my life. They helped me stay motivated just by existing.
Some days are challenging still, though much better than in those first few years. Did you know that any women who are mothers take on additional caregiving for loved ones with disabilities or long-term care needs, beyond the work that we normally do to raise children or to fight through their own rehabilitation? This became the case for me when my mom developed encephalopathy and a resulting ABI (an acquired brain injury) secondary to being diagnosed with Anca Vasculitis. I then also absorbed some of the role as her caregiver. Signing documents in the hospital for procedures and care she needed when she was unable to do so for herself. I took on the role of caregiver and I wasn’t even ready to be back in my full role as a mother to my own children. That was a series of difficult transitions……for all of us. Yet we persevered. Survival was inevitable.
Did you know that the CDC reports that the average life expectancy for women is 81? Living to the age of 81 is nearly four years more than that of men. In fact, many women outlive their husbands. Some even outlive their retirement. Even those on disability. Older, single women face significant challenges in managing their own long-term care needs as well. If you add the extra job of being a mother to all that mix – you learn a lot very fast and you shoulder a LOT of responsibilities.
To be the best mom possible, I realized it was imperative for me to not just let go and let God; but to let go and let others. Let others help me, let others give rides to my kids, help my kids, help my family. Let my husband take on those responsibilities I had as a mom, that I sometimes didn’t have the energy to be present for.
I realized that being a supermom didn’t mean I had to do it all. Being a supermom meant I just had to be here to the best of my ability, to love my kids to the utmost, to voice my tolerances and intolerances in a different way. Being a supermom meant giving myself the freedom to recover at my own pace, and forgiving myself for not being who I used to be. Being a supermom meant being the best me I could be in each moment.
I still love being a mom. I still love hearing the laughter of my children. I love watching them sleep, hearing them play, and watching them grow. I still value being involved, present, all while being respectful of my limitations.
I am still a supermom. I just do it differently. Do you know a mom who is recovering from an injury….who is a caregiver….who is employed…..who is unemployed….who is on disability…..has her own children….or is a mother figure to the children of others….offer to help her out. Can you think of that mom out there who is struggling to do her best? ….Offer to shoulder some of her responsibilities. Appreciate her. Celebrate her as an invaluable contribution to the family as a whole. After all, that is what she is – invaluable.
Is that mother you? Ask for help. Love yourself. Forgive yourself for not doing or being all that you envision all at once, or still. Get involved in a support group, counseling, whatever it takes to help you face each new day and each new moment. You are after all….if you love being a mom….if you are go getter, a survivor, a brave face in a sea of thousands. If you are a mother giving her best effort….even if you aren’t able to do everything….you are still a super mom.
Happy Mother’s Day
~Caren Robinson – May 2019
Below are some articles and links I thought would be helpful to all those who have mothers, are mothers, are children of a mother with special needs, or are caregivers for mothers…..
~ An English-language metaphorical idiom for an obvious problem. difficult situation/decision, or risk no one wants to discuss, or a condition no one wants to challenge. An unpleasant experience. question, problem, solution, or controversial issue which is obvious to everyone who knows about the issue, but which is deliberately ignored because to do otherwise would cause great embarrassment, sadness, arguments, or is simply taboo. ~
What is YOUR “elephant in the room”?
Is it an invisible injury or illness? Have you been diagnosed with a Traumatic Brain Injury?
Is it a Polytrauma you are recovering from?
Is it chronic pain?
Is it Survivor guilt?
Is it lack of sexual libido or change in your sexuality since your injury/illness?
Is it your inability to describe to others what you are going through or have gone through?
Is it the coping skills that you must use and choose to tell noone about?
Is it your bravery, your sheepishness, your courage, your fears?
Is it pride in how much you have acccomplished? How far you have come?
Is it depression, anxiety, or disappointment in your lack of progress?
Is it lack of confidence? Is it overthinking and overconfidence?
Is it your inability to return to the same type of work you used to do?
Is it your desire to return to work, yet unsure of what that picture looks like for you?
Is it caregiver burnout?
Is it provider fatigue?
Is it a source of deep grief, sense of loss, or mourning?
Is it something that you have put in your past and no longer wish to speak about?
Is it something you want to speak about, yet others are ready to move on and not speak about it?
Talking about the things that are bothering you can help clarify them and put them in perspective. In never addressing the “elephant in the room” a general uneasiness, sense of frustration, stagnation, loneliness, and untrustworthy environment can breed a life of havoc and confusion. Break your silence and be blunt in a productive manner. Perhaps even seeking out a therapist to assist you with working through some of the adjustments would be advantageous for you.
Avoiding an issue causes more harm than good….always. When discussing an issue, it is imperative to remain as calm as possible. Using anger or yelling to communicate can absolutely make things less constructive – especially if you are having trouble finding the words to say and the best way to deliver them. Being objective can be super tough. However, it can be helpful if you make a list of facts. Now, when I say facts. I am not speaking about how you feel, how you think, or what your assumptions are. I am talking about facts that you can prove with empirical evidence, historical evidence, and a paper trail.
Keep in mind when talking about that “elephant in the room” that sometimes the very people who need to hear the topic being talked about are the least receptive to hearing it. That often means that person might even be you. Being receptive to talk is important. It is equally as important to actively listen. Support from others that share the same or differing opinions about the issues you wish to speak about will make it not about you, but about the issue and how much it impacts others who have gone through the same thing, or are currently experiencing the same challenges. Support groups (even if they are online) can be an amazing source of support, ideas, and encouragement.
A resolution or plan is something that is accomplished over time. Open communication without apathy, fear, or hopelessness is an integral part of finding what works best for you. Keep an open mind and be willing to have multiple conversations about that “elephant in the room”.
Taking that challenge which is deliberately ignored and opening up a dialogue about it, changing whatever it is that is holding you back from being your best self. This is how to make progress, step outside your comfort zones, and switch an unspoken taboo topic into a healing process.
I have been reflecting. Reviewing old notes, writings, posts from the first 3 years after the wreck. This was the epicenter of the hardest of my recovery. Also the hardest was not feeling listened to by certain providers, especially during that first year; these providers who dismissed my pain, and who I was supposed to be trusting with my care.
I have decided to share some of those thoughts here….in my Blog. This one was from 2014 just after the first of several surgeries to come:
I remember. I remember going to Spectrum Health Butterworth for surgery. I remember the surgeon calling me the night before after weeks of trying to get a hold of him to quash my fears and answer the questions, which to him were probably nonsense….but to me – were the words that drove my every waking breath and desire to understand what I was about to endure.
I needed his reassurance. His candidness. His time. His empathy. His patience and his understanding. I needed his apology, which I doubt I will ever hear. I remember feeling frustrated and angry that he told me to call any time with questions and then never responded to those questions, leaving me hanging perilously from day to day as if I were waiting for my death sentence.
Each moment, perhaps my last with each click of the clock which hung on the wall and taunted me so consistently with each passing hour, day, and night. To him he was probably busy, and thought I should just TRUST him because he was one of the best if not the best surgeon in his specialty/field…..but how could I trust when that trust had been shattered like the pieces that lay inside my body still broken, painful, and damaged?
That trust was broken by him when he didn’t believe me and my complaints of pain, and yet I craved his answers and solace to help me get through the coming days and weeks before that daunting day when I would go beneath his knife. I craved his humanity and his ownership for his role in my current state. Yet that never came.
I felt trapped. I knew I needed the procedure….this surgery. How could I trust once the betrayal had been sown? How could I believe that this was the right thing to do by this same man who cast me aside like a scrap piece of paper not worthy of his time until I got beneath the glaring lights of the cold and clinical Operating Room…..where I saw him momentarily.
How could I in the face of adversity and enormously high risk of dying on the operating table….TRUST?
I took a break, several in fact, and pretended like everything was okay, for my family’s sake. I don’t know how I made it through other than by faith, the driving and enormous desire for relief of the growing pain in my right side (where the ribs never healed) that never went away; and the increased loss of strength and use in my right arm (most likely from forcing myself through therapy for 12 weeks and putting forth my BEST EFFORT with tears flowing like endless waterfalls as I forced myself to continue each exercise…..not knowing that my shoulder/scapula was still fractured and had not healed at all either as well).
How could I push aside the rage and anger that made several professionals miss such an important detail that I was very vocal about? How could I give in to the experience when I had so much left to say, learn, live, and experience?
I just kept breathing…..deeply, slowly, studying each item, each line in the ceiling as I was wheeled along in the stretcher. I focused on the names of those pushing me, and their conversations and attempts to bring calm to me. I embraced each quirk on the face of my husband, mother, and Medical Case Manager as this may be the last things I see. I was acutely aware of every single detail and overwhelmed by the voices, noises, and conversations around me. The lights were bright, my headache grew, and I had to take myself to another place while still being exactly where I was. I know that sounds silly but I have no other way to explain it..
This fileting of my body with a magnificent dance of his scalpel tools and his skillful artistry beneath the clinical shroud of the operating room; a handful of specially trained staff who would bring me to the other side of waking up once more…..or so I secretly begged for – and perhaps begged for aloud as well.
I remember putting on my bravest face and not knowing if this was the day that I kissed my children goodbye for the last time before I saw them walk out the door to go to school; not knowing if this was the last time that I would see my mother’s face, feel my husband’s touch, and I was so afraid. I wasn’t afraid to die. I just wasn’t ready. I thought on this intensely. Should I have written good bye letters the night before. I had decided not to because to me that was the same as giving up. How do I find the words to say the things that I feel? HowI do I make the words in my head come out on paper in the way I wanted them to and to have enough of an impact to make everything up to that point feel “worth it” when since the wreck I struggle just to get my words to get from my head out my mouth in the way I desire.
How do I trust God and the Universe and all my spiritual beliefs and experiences? How do I know at this point that God is even real any more? Then I had to remind myself of all the miracles surrounding the wreck and force myself to believe that miracles would happen that day.
As it so happened…..the 3.5 hour surgery we were told it would take turned into about 8 including the 2 hours in recovery, per my husband and mom. The stakes were high. The man I decided at the last minute to trust with my life in its entirety took me on a journey and he and his team brought me out the other side.
This was my first post surgical feeling of gratefulness!!! When my eyes opened and I noticed people rushing around me in recovery, and seeing my O2 sats in the 80’s but just feeling such calm, feeling peaceful, acutely becoming aware again, and just blinking ever so slowly…….grateful in that very moment. Grateful that I had been allowed to once again survive that Journey…..
I am a Survivor trying to bring inspiration and awareness about Polytrauma and TBI to others.
33 Months ago, our Website Page for YOUR STORIESwent LIVE. Since then, we have met some amazing folks and had the opportunity to share their stories, experiences, and soulful expressions with all of you out there.
If you have not submitted your own story. You can do that by starting HERE.
Survivors, Caregivers, Providers; Parents, family, or friends – share your story to be published on this site today. We are glad to help you in any way we are capable.
We have recently finished Stories for various folks that we would like to share with you. Take a look, read some, leave a comment at the bottom of their story if you choose, and pass the link on.
Let’s bring Global Awareness to Polytrauma and TBI
This is an important second test in settings where CT or MRI are negative after a closed head injury with post-injury neurological or psychiatric symptoms.
Hermitdom – In the beginning, not only did I NOT want to leave my house to venture out into the outside world, I often was absolutely content to remain in my bedroom where I knew what to expect and it was somewhat controlled and felt safe and comfortable. This was my safe space. Safe from the bright sunlight, safe from too many people talking at once, safe from the general noise of the world outside the room, safe from traffic, safe from having to explain what was wrong with me, safe from having my daily emotional breakdowns in front of others, safe from trying to stay awake, safe from being looked on with judgement or pity, safe from healthcare providers appointments, safe from additional pain from moving broken limbs across the room and down the stairs to face the reality I did not seem to fit in any more.
As time progressed, as my healing progressed, as I was forced out of the room due to sheer necessity to survive my pain, to attend numerous therapies and medical appointments, and to be a parent – I began to adjust to new tolerances. I also learned rather quickly most of what triggers to avoid so I didn’t end up in a full blown panic and puking my guts up from the dizziness, headaches, and a bouncy massively overstimulating environment.
Getting out of the house is a solid accomplishment. There is a lot of planning that goes into getting out and about. There are things to consider that I took for granted before the Polytrauma. Checklists are my friend. If I deviate from this process we have established, things do not go well at all.
Some days I do better than others. I find I am able to be out longer and more often than even a year ago. However, I recognize that I do not have the same comfort level I used to before the polytrauma and I value getting back home as soon as possible. Some days I still have to force myself to leave my room or go downstairs to the main living area of our home. Some days I feel ready to face the world, get outside, something happens that I didn’t expect and NOPE…back home I go.
Trips away from home, the longer the day, the busier the activity, the longer the recovery time afterwards. A one day trip could take several days to recover from. A day of appointments could take a week to level out from again. If you have back to back appointments or requirements, it becomes a vicious cycle of feeling overwhelmed, incompetent, and beyond exhausted – just weary and pummeled.
So planning in advance, if possible, become a requirement. Having someone help you organize your schedule, your time frames, your goals is imperative to attaining those small victories.
Having things to help you cope in moments you can’t be home is imperative.
Brain Time – I created this term with my family. I wanted desperately to spend time with my kids, my husband, our friends, and people in general. I wanted desperately for things at home to be normal. Since the polytrauma I would feel emotionally and mentally….well…..flooded. Like I was standing in the ocean and wave after wave was hitting me in the face and taking my breath away. In my case though, sometimes their voices all at once, their walking, their questions, their playing, their presence is enough to overwhelm me. It is like there are too many sounds to sort out or too many thoughts to try and think at once. I would become irritable, frustrated, nauseas, and when I wanted it to stop…. it literally had to stop NOW, or I would puke, have an emotional crying meltdown, or just freak out. So we came to an agreement that if I said “Brain Time” all things ceased no matter where we were.
In the beginning I was at the point when I couldn’t easily reset myself, so I would say “BRAIN TIME”, go in my room (or they would have to leave my room), and I would stay there until things settled down in my head. No interruptions, no calls, no questions, door shut. Sometimes this was moments, sometimes minutes, often hours, or occasionally days. I needed absolute silence, a dark room, a warm heavy blanket and to lay down perfectly still. I slept a TON.
As time has passed and I am now three and a half years out from my trauma, I still call BRAIN TIME now and again, yet it is less often that it used to be and I have employed other coping mechanisms to help me reset myself.
However, once my brain has decided it has had enough for that moment, or that day. It’s like it’s done “now” and not even I can control the shut down process. I am learning to pace myself still and manage this more effectively. This does not make for a great social life though, I will say that.
Directional Instability – Okay I gotta say I have always been the type of person to have a pretty decent sense of direction. I never had a problem getting “lost” when I went into a building, when I drove, or when I was walking somewhere. I was always quite proud of this “inner compass” and it served me well in marching band when I was a teenager, in college and in my work life, when driving an emergency vehicle, when locating items others seemed to struggle finding, and when driving my personal vehicle.
After the polytrauma, it was like someone took that inner compass and smashed it. When I tried to lift my head, the room would spin like just got off a tilt-a-whirl on the Gravitron from a carnival. When they would sit me (and eventually after I sat up on my own) I would be so enormously dizzy that sometimes that labyrinth of puking was unavoidable. No to mention the throbbing headaches that seemed to be everywhere and made my forehead feel like it was 50lbs all by itself pulling me forward. The back of my neck ached and I would often have a “belly ache in my neck” if that makes any sense. Looking up and left exacerbated EVERYTHING and so I learned to avoid looking that way.
Two and a half years after the trauma I started to return to driving. I would learn my inner compass was missing/broken. I was horrified to find myself LOST after taking my kids to school. In fact, I couldn’t remember how to get there….a trip I had made hundreds of times before. I used a GPS because it was like I had never been there before. Now THAT made me feel coo-koo….I didn’t understand. Then I got lost heading home. I literally ended up 20 minutes in the opposite direction because I couldn’t remember what to do or how to get where I needed. GPS became an absolute crutch. As time has gone on, I have gotten better about figuring out my routes. Often times I could think of where I needed to go…yet applying it to real life outside my head was a different reality entirely.
It is a horrific and scary feeling to feel LOST. I called my husband in tears a few times telling him I didn’t know where I was or how to get home (when phone died and I didn’t have access to GPS). Most times he would answer the phone, sometimes he didn’t hear it and I would be out there in a full blown panic. I would feel scared and the noise around me seemed to get magnified to a level that felt like it was trying to kill me. I could feel myself slipping into this dark space of isolation and I literally couldn’t think of how to fix it. I do not remember how I made it home in those elevated panic times. What I do remember is deciding I couldn’t drive yet and that I didn’t feel safe outside of my house, let alone my room. It has been a massive process to get back to driving again.
Now I am driving more often and the short local routes I do really well at. If I forget I just turn on the GPS. We purchased a charger for the vehicle so I never have to worry about my phone dying (unless the bill doesn’t get paid – GPS doesn’t work then by the way). So the phone is as important as the mortgage for me as far as financial priorities.
Buildings I have been to a lot I still get turned around in since my Trauma. Oddly enough sometimes I get lost in my own neighborhood or kids’ schools. If I survive an outing without getting lost, having a panic attack, or struggling to survive the experience – I consider that a WIN!
Peat and Repeat Languaging – the way I communicated became annoying and complicated. I not only would have to read numerous times a sentence or a paragraph to catch it all, I would also have to listen to a voicemail like 4-5 times to get it all because remembering the number or message seemed suddenly impossible. When people would talk to me I had to have them look at me to hear them. I found myself reading lips to understand what I was hearing, or thought I was hearing. If they turned their backs to me I would ask them to turn around and repeat what they said. Some folks are super accommodating, some act put out by this. Often times folks think you aren’t interested in listening or you do not care about what they said. It wasn’t that, I just couldn’t process what they were saying. Sometimes the words didn’t make sense. It’s like I was listening to a foreign language sometimes. Sometimes it was like I could see their mouth moving, hear noise coming out, yet couldn’t make out the words. This was maddening. Oh! if I was doing something and all my focus was on it (like typing or reading), forget about me hearing you..it just didn’t happen.
This has gotten better for me in a lot of ways through my rehabilitation journey, not better in other ways – however, I keep learning ways to cope with it despite its abounding annoyance. I am a lot better about being vocal about it though with who I am speaking to now. Once you get used to functioning at a certain level it just becomes your new normal and you accept it as what is.
Where’s the Word?… Doh! – Okay, I have always been a talker. I started talking early as a baby and I haven’t quit since. I love words, their meanings, and expressing myself in a creative fashion. I won spelling bees in my younger years and have always been a semanticist and quite loquacious.
However after the trauma, that seemed to also have changed. I couldn’t remember how to spell basic words. I find myself misspelling things often and missing the same specific letters when I type. I would look at say……a couch. I could see the word in my head, I knew what it was, yet all I could get to come out my mouth was “that thing there that we sit on”. I have become accustomed to calling things differently than what I am thinking now or what they actually are. Sometimes I come up with some pretty creative descriptions.
Bon Appetit No More – Food has been my friend for years. My family has always celebrated with food, rewarded with food, and used meal times as a social gathering time to express our love while being able to share something we all enjoyed….cooking, talking, and spending time together. I could always tell when I was hungry, when I was full, and when I was snacky.
After the polytrauma I seemed to lose the ability to feel hunger or fullness. For some bizarre and I am sure possibly scientific reason I lost my appetite or desire for food in general. No more interests, no more favorites, no more “cravings”, and no more enjoying the things I used to enjoy before. My sense of taste and smell had changed. Some of the things I enjoyed before now repulsed me. Smelling certain types of food cooking was enough to turn me “green” (sick). Just looking at certain types of food was repulsive. The connection with food emotionally seemed to go on vacation. In fact, if I wasn’t brought my meals in those early months and sometimes still…I just wouldn’t eat because I would just forget to eat or have no interest in it.
As time has progressed, every once in a while I go from no appetite to suddenly HANGRY (angry rage filled hunger – almost a desperate hunger); HANGRY is rare though. More often than not, I forget to eat or have no interest in eating.
I do like some textures or flavors of some things that I never liked before. My family and I equally find this as quite bizarre.
What Temperature Is it Anyway? I remember a few specific things during my recovery process that stood out and I still wrestle with. Chronic pain I have written about in other Blog posts and will probably write about again….however what I am referring to here now is TEMPERATURE. More specifically FREEZING MY TUCHUS OFF!!! I was always cold. I couldn’t get warm, not even in the Summer months. People would be sweating and I would be freezing and covered up with my electric blanket and shaking from being so cold. I gotta tell you that being so cold that you are shaking and having multiple fractures does not a good combination make!
I have come to realize that my thyroid-pituitary-hypothalmus axis was way off. My hormones were all over the place and apparently I rattled that temperature control center of my brain pretty good.
I still have some great hurdles to overcome when controlling my comfort regarding temperature. At least now I can feel warmth eventually and not be as cold. Sometimes, I even get hot flashes occasionally and naked isn’t naked enough to cool down. More often than not though, I still get cold. Brrrrr’kin is what the kids call it.
So what temperature is it anyway? I am probably not the most reliable person to ask. You might want to check outside…..then let me know.
There are many more nuances that go along with recovering from a polytrauma and these “7 exposed mysteries” are not an exhaustive list, not even for my experiences.
However, they are some of the things that are not necessarily visible changes to anyone who isn’t experiencing them directly and I felt they were worth mentioning. If you are experiencing these things, you are not alone. What you are experiencing is real.
Hopefully, understanding that this is now your new normal will help you accept yourself as you evolve towards your plateau in search for treatment and healing.
The answer to that questions is quite simple for me. it is a resounding and emphatic YES!!!
I am so eternally grateful for the No-Fault system. I sustained a Polytrauma which included multiple orthopedic fractures (5 in my spine alone, ribs, wrist, pelvis, scapula/shoulder, soft tissue injuries, nerve damage, and a traumatic brain injury).
Thanks to Auto No Fault I was able to have the necessary MULTIPLE xrays, CT Scans and lifesaving surgeries to help me survive. I had to go out of State to save the use of my arm due to a shattered scapula as we have no Trauma surgeons in Michigan who were trained to do that repair. Michigan No Fault made it possible for me not to lose all of the function in my right arm. My whole scapula and shoulder had to be rebuilt.
Medicaid and Medicare would NOT have covered this. We would have been stuck in months of pre-authorizations and appeals and I would have died.
I would have left behind my husband (who is also my provider so I could remain at home and not in a nursing home) 6 children, a mother, a brother, a
nephew, and other family. I would have lost the ability to advocate for others and to function at the level I currently function at.
My story would have ended tragically. My story, while yes, tragic and traumatic continues to be HOPEFUL due to Michigan Auto No Fault.
I WILL need surgeries in the future. It isnt IF….its WHEN. Auto No Fault provides me with the medical security to still be here for my children, and hopefully some day….their children.
Please, I implore all voting members to vote
NO ON HB5013
YES on the Fair and Affordable No Fault Reform Plan
You are literally investing in Michigan’s future and survival by voting to save lives and protect the communities you are pledged and voted in by your constituents to serve.
What do you want your legacy to be as a politician, as a fellow human being leaving their mark on this world???
Someone who saved lives and cuts costs by holding insurance companies accountable, or someone who sentenced thousands of men, women, and children to death and financial ruin?
You can be the implement of positive change. You can be a hero. You can be a HOPE’ster.
NO ON HB5013
YES on the Fair and Affordable No Fault Reform Plan
What Exactly is “Standard of Care” as it relates to the medical community?
The “medical standard of care” is typically defined as the level and type of care that a reasonably competent and skilled health care professional, with a similar background and in the same medical community, would have provided under the circumstances that led to the alleged malpractice.
A diagnostic and treatment process that a clinician should follow for a certain type of patient, illness, or clinical circumstance.
The level at which the average, prudent provider in a given community would practice. It is how similarly qualified practitioners would have managed the patient’s care under the same or similar circumstances.
I have learned over my entire life through various experiences; also being in the medical field for most of my adult life as a healthcare provider in some way, shape, or form that the Standard of Care is as varied as each personality that goes along with the person representing that Standard of Care.
When I had patients I always tried to give them the best of me and my knowledge of my acquired training at that time. When I came across something I didn’t know (which was a continual learning process for sure)…. I immersed myself in learning about the things I didn’t know how to answer for what I was specializing in at that time. That was my way of making sure that I didn’t have that same issue come up again. I guess I just assumed (yes, we know the misnomer of what assume means) that this is how all people sought to learn when they had a passion for medicine. Specialists in a field even moreso…beyond the norm even.
Specialists, surgeons, Department heads I guess I always expected more of those folks. Surely they kept up on all the latest trends, the newest studies, the symptomology associated with the topic(s) they specialized in. Surely they could spot a problem, would assure that the best outcome for the patient was acquired, especially in favor of positive outcomes with their name attached to it.
Surely I could look at them, listen to them use my voice to communicate with them, and trust they knew what they were talking about because after all, their fervor and thirst for knowledge was above and beyond what the average medical professional entailed. Certainly more than what I was trained to know.
So it only made sense that on that fateful day when I became the voiceless patient, clothing cut off to stark nakedness in an emergency room with massive injuries, multiple broken bones, head injury, and clinging to life with each labored breath…..that the sheer mechanism of injury (severe car wreck with ejection and other driver pinned and needing to be cut out) should have demanded a certain Standard of Care from every provider I came into contact with, within that first year, and every day after that.
I have had some really great providers. I still have some great providers. I want to say that first. There are a handful who have done their due diligence and even exceeded the Standard of Care. They are the ones that listened. That actually enjoyed their job and their patients. They are also the ones that keep up on the current and updated things in medicine, ironically enough. They are the ones who think of ways to make things happen instead of making excuses of why they cannot make things happen. They are the providers that never give up on you and take risks to better your quality of life. They are few but mighty. These are the providers I have learned a lot from and have enormous respect for.
The providers who fell short on their Standard of Care, or didn’t even attempt to live up to it….. Those providers left me impacted in ways that created a ripple affect that delayed my care, caused me further injuries, and exacerbated things for my recovery process….and not in a positive way. They are the providers who didn’t listen. Who jumped to conclusions based on opinion rather than facts. They fed off of other reports by other providers that also did not care, did not document properly, or dropped the ball in some fantastic and important way; perhaps even adding wording that invalidated the injuries that actually were quite legitimate and yet ignored. These are the providers that I felt I knew more about my care and the latest treatments available than they did (yes even if they touted themselves as specialists in that field). These are the providers I lost respect for, or never had the chance to establish such for.
The Standard of Care cannot be overstated in its importance. If you specialize in a field, learn all you can about that field. Study it, know it, and be willing to learn more about it. Medicine is changing daily and if a patient brings you the current studies, be grateful. If they discuss them with you and you have never heard about them, go look them up and research them yourself. Knowledge can only make you better at your craft. If you cannot listen…truly listen to your patient when they say they are still suffering – you are in the wrong line of work. Go on a quest, do no harm, and advocate for your patients.
The Standard of Care echoes through many professions, yet in this particular post we just address the medical view as a patient, medical advocate, a Survivor.
A HOPEster is anyone who is interested in helping one person succeed to be independent – even if the person they are currently helping is themselves (specifically related to Polytrauma and Traumatic Brian Injury – though can apply to anything other than these two things as well).
A HOPEster is someone willing to share information, offer support (whether that be emotional, mental, physical, or just by sharing awareness information), and encourages advocacy (self-advocacy, medical advocacy, advocacy awareness).
A HOPEster is someone that thinks outside the box, is passionate, idealistic, and believes in the inherent goodness of others and our collective responsibility to each other as human beings.
(right click on picture to save to your device or share link in above web browser)
Hello There HOPE’sters. We are thrilled to announce 2 awareness ads for this website for you to share in emails, in your social encounters both online and offline.
Below each video is a description of what the video is about and why it was created.
Feel free to click the “SHARE” button in the top of which video you like the best, to choose the sharing option you prefer. SHARE SHARE SHARE….help us bring awareness to others.
This one was created with the thought in mind of how we can overcome anything with the right attitude, with awareness/education, and with proper support. Support can come in the form of friends, family, providers, and even our own children. It is important to remember to find our smile, to love, to laugh, and to embrace life and live it to it’s fullest – in spite of our seeming limitations and new realities. That, in the end, we will be okay – because we have each other – we will overcome!
(of course bubbles always represented to me, a time of innocence, frivolity, and life’s possibilities – you never get too old for bubbles)
This one was created first and the song’s theme is “I will fight for you”.
I created this website with the idea of healing and fighting for myself and my recovery by learning and documenting as much as I could about my injuries…and then documenting what I had learned from my own experiences, documented research, and subjective interpretations. I created the website with the desire of helping to fight for others with similar injuries (polytrauma or traumatic brain injuries) and help bring Awareness to as many people as possible. I want it to be a global reach that says:
“Hey, you are not alone out there in your recovery. You are not alone as a caregiver or a provider – you are not alone with the questions you have, the symptoms you feel, and the life you are struggling to make work for yourself or others”.
I want this video to be something that is remembered. Whether you hear the words “I will fight for you” as a song to yourself in your own mind to help you keep going – because your life is truly worth living; or as a representation of your desire to support and advocate for others….that you will fight for them, no matter what; or as a reminder that this site is a place you can come to share, get information, and feel like you are in a place that cares and understands.
The blooming flowers in the video are Cherry Blossom Trees. This has been symbolic for me for quite some time now. See our page under CHERRY BLOSSOM TREE PICS.
(any ideas or comments welcome – please post them below or email us through our Contact page)
Unless there is objective evidence of brain injury on MRI or CT Scan (hemorrhages, hematoma’s penetrating skull fractures into the brain, etc) people assume the individual expressing symptoms of a traumatic brain injury is faking, exaggerating, or malingering their injuries or the person has psychological problems that had to have pre-existed before their accident. The reality is that the majority of mild (mTBI) and moderate brain injuries show normal results on an MRI and CT scans. They do not show diffuse axonal injuries nor do they show levels of intelligence. Keep in mind also, that women also tend to have longer recovery times than men with regard to brain injuries as shown in recent studies.
Diffuse axonal injuries (DAI) are caused by acceleration, deceleration, and contact forces. DAI affects individual nerve fibers which can lead to a disruption in nerve communication. DAI is microscopic damage to the axons in the brain neural tracts, corpus callosum, and brainstem, is associated with significant mortality and morbidity. When these forces are great enough it creates a shearing force that severs the axons of nerve fibers, which causes nerve cells to die and can create swelling in the brain. The main symptom of diffuse axonal injury is lack of consciousness, which can last up to six hours or more. A person with a mild or moderate diffuse axonal injury who is conscious may also show other signs of brain damage, depending upon which area of the brain is most affected.
Diffuse axonal injury causes cognitive, physical, and behavioral changes that compromise social reintegration, return to productivity, and quality of life of patients and their families. These changes persist beyond the acute phase of treatment and continue for a long period after the traumatic event. Diffuse axonal injury, and more generally TBI, often results in physical, cognitive, and behavioral impairments that can be temporary or permanent.
Due to the diffuse and microscopic nature of the injury, CT scans and general MRIs are typically negative unless small areas of bleeding within the brain are noted within the cerebral cortex or corpus callosum (tracts of white matter in the brain). If a patient presents with unconsciousness and these tests are negative, the medical facility should move onto a different imaging technique to check for DAI. Depending on the severity of the injury and the extent of the damage. A concussion can be considered a mild case of shearing brain injury. At its mildest, DAI can occur unnoticed.
Someone with diffuse axonal injuries that don’t’ show on an MRI or CT scan may also have brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.
The occurrence of DAI depends on the mechanism of injury; it is more common in higher energy trauma, especially traffic accidents. Someone who has incurred high velocity trauma, blunt force injuries, or multi-system traumas often have post-traumatic amnesia (PTA). PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage.
A brain injury does not necessarily affect intelligence. Intelligence is a stable trait which includes many aspects of cognitive functioning. Following a traumatic brain injury, the brain is unable to function as well as it did prior to injury. This is why we typically see some difficulties with memory or academics. However, once the brain recovers there is no change in a person’s overall intelligence. Your intelligence is based, depending on the definition of intelligence, on the son total of your knowledge.
Someone’s IQ can be unaffected by a TBI, but other parts of the brain that “pilot” or guide one’s brainpower can be messed up. Decision-making and complex social interactions can cause major problems in one’s life and career. The individual with high intelligence may still have cognitive problems such as headache, difficulty thinking, memory problems, attention deficits, mood swings and frustration. These injuries are commonly overlooked, especially in those with high intelligence. Their low threshold of functioning or slower processing speeds may appear as average where prior to injury they would have tested as above average..
The brain of the intelligent person is more complex in appearance, not as soft, and has greater weight relative to size. Additionally, it can be noted that the intelligent brain may have an enlarged prefrontal cortex or parietal lobe relative to other areas of the brain. More intelligent people have more wires, more connections and more complex architectures in their brains. These are reflective of genetics, as well as developmental experience. Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.
That being said, Intelligence and personality dysfunctions after minor traumatic brain injury (TBI) (whiplash; slight head impact) incurred in a motor vehicle accident (MVA) were studied in adults after an average interval of 20 months. There was a mean loss of 14 points of Full Scale IQ from estimated preinjury baseline IQ determined from the standardization group (WAIS-R) without evidence for recovery. Personality dysfunctions included cerebral personality disorder, psychiatric diagnosis (30 of 33 patients), post-traumatic stress disorder, persistent altered consciousness, and psychodynamic reactions to impairment. Cognitive loss is caused by interaction of brain injury with distractions such as pain and emotional distress. Unreported head impact and altered consciousness at the time of accident contribute to the underestimation of brain trauma after minor TBI.
Just one concussion can lead to a decrease in brain volume, according to a new study in the journal Radiology.
Specifically, researchers from New York University’s Langone School of Medicine found that people who had suffered a mild traumatic brain injury and experienced symptoms of the injury a year later also experienced brain atrophy (brain shrinkage).
“This study confirms what we have long suspected,” study researcher Dr. Yvonne W. Lui, M.D., assistant professor of radiology and the neuroradiology section chief at NYU, said in a statement. After mild traumatic brain injury, “there is true structural injury to the brain, even though we don’t see much on routine clinical imaging. This means that patients who are symptomatic in the long-term after a concussion may have a biologic underpinning of their symptoms.”
Researchers specifically found that those who had sustained a mild-traumatic brain injury had less brain volume in regions linked with anxiety, memory and attention problems.
The bottom line here is that you can have a mild or moderate Traumatic Brain injury with long lasting debilitating symptoms and still have the same intelligence. You can have a severe traumatic brain injury with empirical radiological evidence and still maintain your intelligence. Brain injury does not equal lack of intelligence. A person’s intelligence is not a solid basis for deciding a person’s extent of disability after an injury.
The High IQ TBI (a blog which is worth the read about high IQ and TBI – this will take you to a different site)
I really do not like the question “what do you do all day long?”
It differs so much from day to day and moment to moment that having a schedule is sometimes a curveball I miss catching; so there is no simple answer.
Before the wreck the answer was a lot more simple. Before the wreck it was wake up and get kids ready for school. Run errands, set appointments, pay bills, clean, organize, manage the household schedule, keep track of the budget…all this before I went to work for an 8-12+ hour shift. Come home check homework of kids, enjoy the family or deal with family drama (any day is a toss up with kids truth be told). Deal with all the things that comes with having a blended family, in-laws, and being a working mom and stepmom.
In my life before I would often be described as independent, bold, courageous, strong-willed, determined, a goody two-shoes, ethical, self-conscious yet perfectionistic, accomplish anything I set my mind to; a great multi-tasker, and adventurous.
THINGS I DID BEFORE: I was involved in my kids schools activities, field trips, PTO’s, on top of my full time work life. On top of all that Rick (my husband and I) managed to still do stuff with the kids and with each other away from the house. Though I have to tell you work was the main part of our lives as we both worked full time+. I loved to drive. Man did I love to drive. I even have my motorcycle endorsement (yep even used to own two of my own motorcycles before I met my husband). I loved going to the movies, the beach, museums, comedy shows, community events, carnivals, fairs, and other community events/fundraisers. I had a life that made me feel fulfilled and though stressful, exhausting, and full – nothing that a good night’s sleep, a warm cuddle, a payday, or a homemade dinner couldn’t fix. In some ways I believe I wore rose colored glasses and saw the potential and possibility everywhere. I also had a LOT of responsibility and my husband always referred to me as his “walking filing cabinet” (cuz I rarely forgot anything and knew what was going on when and where). I feel I always survived grief and stress with some kind of grace.
FAST FORWARD TO AFTER THE WRECK…..
A total cumulative time in the hospital as a patient 6+ months, literally 100’s of medical appointments, 4 surgeries, 100’s of therapy appointments, tons of labwork, and radiology galore. Near death experiences. Enormous and unwavering pain in ways I never imagined feeling such pain. A complete stripping of the body, soul, and mind through harsh realities about how the world works…..or rather doesn’t work if you are in a position to depend on it for your day to day survival.
Pain pain and more pain. The pain is so much that after a while you build a new tolerance to where the pain exists for so long that you almost don’t notice it because it is so much a part of you that you don’t remember the last time you didn’t have it. Then another surgery brings some relief and you get excited and become hopeful and then BAM something else pops up, or it flares up. All of a sudden, you wake up one day and realize that you are depressed, angry, about all that this “wreck” has seemingly taken from you. You find yourself so deeply exhausted, fatigued, and emotionally overloaded EVERY DAY that you want to cry but you have no tears….only sadness and a feeling of defeat. You look at yourself and you wonder what happened to that busy person who seemingly did everything. Where did she go? You entertain dark thoughts that you keep at bay because if you focused on them they would surely overtake you and swallow you up. Radical acceptance is painful you realize. Accepting that your new limitations, your memory problems, your scattered disorganized, lack of focus, emotionally mercurial self is your new normal. Suddenly you have all these rules about what you can and cannot do, why, when, and yet you keep pushing yourself anyway. At what point does the emotional overload – overload you to a point of no return? Every time I feel I cannot take any more…more is given to me by my body, or the universe that pushes me further down the rabbit hole.
The harsh reality and unspoken truths that no one really talks about as your healthcare provider….is that after extensive injuries is how the picture of your sex life changes dramatically; they don’t tell you that your social life, your work life, and your sense of self identity (unless you fight like hell to stay afloat) all changes; but these are real things that I think about.
Will I ever be able to return to a job again? Will I ever be able to think and function like I did before? Will I ever get my memory back? What does my future or life expectancy look like? How can I get value from the life I have now? How do I get away from living a life that I don’t truly get a sense of accomplishment from? How do I live a life for myself that has meaning, value, and matters? How do I not give up when the obstacles seem so impossible to overcome? How do I be for my kids, my husband, my family, what they need me to be – when I don’t even seem to be enough for myself? How much am I willing to do today which takes away from what I can do tomorrow.
I often think how would people describe me now? Brave, a miracle, survivor, pessimistic , emotional flooding, anxiety, impatient, forgetful, hurting, impatient, boring, scattered, obsessive and compulsive, lacking filters, insecure, intolerant, and riddled with panic, PTSD, irritability and feeling extreme waves of helplessness in this enormous sea of HOPE, love, and a desire to overcome, heal, and accomplish.
That me….the one who longs for normalcy….THAT woman seems further and further from my reach some days. Stricken with a deep-seated grief process as my childbearing days have surely come to an abrupt and non-consensual halt and the barren feeling and realization that having any more children would be dangerous to my body and would also require some kind of bodily performance that my body has seemed to have abandoned and I have been in deep grieving about. You know that song called “Someone that I used to know”…..yeah that is pretty much how I feel about sex right now. It’s how I feel about the ability to be a person who has to let go of the idea of bringing new life into the world. It’s also though how I feel about how I identify with myself as this person that exists now only in the shadows.
Here I am….and here is one more thing that the wreck seems to have stolen….. that level of intimacy from my marriage dented…that changed the dynamics of our relationship.
Take, take, take. These injuries just keep taking from me and my family. I need to change my thinking I tell myself and I do; I change my thinking. I need to change my direction I keep telling myself…so I focus on helping others going through this kind of struggle.
THINGS I DO NOW: Sleep, home therapy programs, medical appointments, research my medical stuff, blog to help myself and others with Polytrauma and TBI, sleep, cope, be the best mom and wife I can with where I am at right now (which is not even close to where I want to be), more activities as my body will allow, and did I mention sleep?
Knowing I HAVE to go in a direction of mind and body positivity to stay motivated (huh…what is motivation?) and having no clue how to get there is very lonely and makes me feel lost sometimes.
I have to be kind to myself in order to move on. Dancing through the dynamics that each day brings is sometimes seemingly impossible. Yet somehow, someway between each excrutiating headache or spasm….I scrounge, pillage and plunder and find a wee bit more courage to get me through the day.
Defeat, Depression, cycling grief and a dedicated struggle to excel and never give up – the unspoken truth of emotional overload from a Polytrauma.
So hello there soul searchers. There has been a lot going on with my body and my life over the last 3 years. I have gone from calling it “my wreck” to “the wreck”. For the longest time it called it “my wreck” because it was something that had happened to ME. However, in my effort to step outside of myself and towards recovery away from a “patient” status and more of an “advocate” and “self-advocate” status – I want to try and keep myself somewhat separated from it as I do not own it as my own, but rather something I experienced.
Anywhooooo, that being said, I have definitely been forced out of my comfort zone the last 3+ years with my body. I have learned to get naked, show owies, show scars, and talk about taboo topics with specialists, providers, and support teams to the point that I can pretty much talk about any topic regarding my body without it being a “hush” topic. In fact, in this whole time since my wreck noone asked me about my menses, aside from my previous PCP Dr. Mathias (a staunch adovocate for me) who I think at this point I have Martyrized since she moved out of State….or ….I should add, noone that I remember anyway. I gotta allow room there for that possibility. I can say though, that if anyone asked, they never did anything about following up on it.
The body is a marvelous piece of art and machinery. For a woman, when she experiences a great bodily trauma, especially involving a Traumatic Brain Injury (which is a different recovery process for a guy by the way – sorry guys) – there is a whole host of things that come into play that most doctors and specialists do not even address, though it is absolutely critical to do so.
Did you know? Now here is where it gets super personal so you may not want to read past this point…….
My menses was mostly irregularly-regular before the wreck. I was due to start my menses between January 7-10, 2014. I was in the wreck on January 4, 2014. Now you may be thinking wow thanks for sharing information I didn’t need to know. Why does this matter to me as a reader? Good question!!!
Did you know that I did not get my menses between the 7-10 of January? In fact I didn’t get any menses at all until mid July 2014 which was not a full cycle of days for me. Then I skipped some months then a couple of months I had my menses THREE times….(yeah that was a pain to deal with as I had someone doing all my pericare at that point still) in ONE month. Then a month with only a two day cycle and missed more months and this continued for about 2 years or so. It wasn’t until late 2016 I started to get back to a somewhat predictable cycle.
Did you know what during this whole time in 2014 and part of 2015 I was losing handfulls of hair, like literal handfulls and my hair started thinning out. I had no apetite, no liido and lost just about 55lbs in a 10 month span of time. My medical record documents me bringing all these issues to my providers. Like literally all of them. Noone knew what to say except sometimes the body “just does that”.
Well, except Dr. Mathias, PCP who said she felt I most likely had hypopituitarism and hypogonadism and that my pituitary and hypothalmus had been damaged by the Traumatic Brain Injury. She suggested I make contact with a Neuroendocrinologist. Lo and behold, no Neuroendocrinologist in the whole State of Michigan….go figure.
My weight held and I even lost a little more until the Spring of 2015 when suddenly over about a 3-4 month span of time I gained nearly 50lbs back and then another 10 then 18lbs subsequently. I then started growing hair in places that hair shouldn’t grow on a female and I was mortified. What was happening with my body. I still had little appetite and I don’t remember the last time up until that point that food sounded interesting at all.
My thyroid labs and other labs were all over the place, yet noone thought to check these the whole time I was hospitalized (nearly 4.5 months). Even though my medical records showed a preexisting Hypothryoidism, noone ever did a thryroid panel on me – isn’t that bizarre?
I have been battling many neuroendocrine changes as a direct result of my Traumatic Brain Injury and bodily trauma from the wreck and nobody did due diligence to catch this. Yet all my symptoms were documented in my records. Documented but not followed through on. Again, bizarre!
Recently in an online support group someone brought up that they hadn’t had their menses for months since their TBI and wanted to know if anyone had experienced such a phenomenon. Suddenly the comments came flying in. I was astounded. Then I started to research.
How different would my rehabilitation plan have been, if I was tested properly, with some pretty basic and inexpensive blood work while hospitalized? I can tell you that I have been chronically anemic since then. My labs are still all over the place with a lot of things. When I brought this up to a recent provider, they said they didn’t think my menses stopping had anything to do with the wreck and they couldn’t explain the hair loss and other symptoms – that it was just “coincidence”. Wow – really? Turns out they couldn’t have been more wrong.
Here is a link to the compilation of the research I did regarding this very topic:
As it turns out, there are a lot more studies out there than I could even begin to fathom. So why was something so well studied still not a matter of automatic testing in a level 1 trauma center of all places…or beyond?
As it turns out, me being within 2 weeks of starting my menses (within 3-6 days of it actually) is absolutely clinically significant regarding my rehabilitation overall. See link to see why…….
Amazing stuff…..the search continues!
Please comment below and share this post with someone. Let’s spread the word and bring awareness.
Just wanted to post that we have completed another page on our Website here to assist you in getting some answers.
I just want to note that I have been chronically anemic AND have had continually low Vitamin D counts since the wreck. In fact while hospitalized within those 3.5 months after the wreck, my Vitamin D was less than >1 (not even readable) – crazy huh?
I have been on lots of Vitamin D supplements since the wreck too – D2 D3 and Calcium+D….so Deficiency Def Trauma related!!!
Inquiring Minds want to know: What were your injuries?
I always wonder if they want a full answer. Sometimes it seems too much to talk about so I just say “polytrauma”. Sometimes this is sufficient. If not, it will lead to more questions that are almost always more specific.
Believe it or not I finally have most of this list memorized now after 3 years. However, I still always leave something out when talking to someone and trying to determine what to tell what specialist or what is important to mention or what wasn’t….this was not only overwhelming but impossible.
My family had kept track of injuries as they were discovered and this is their list in addition to mine once we started combining them and matching them with Medical reports we had. These are the injuries from the 2014 wreck in chronological order of discovery. The list is great because I just add to it as things are discovered and then just provide the list to my providers when I see them. It also saves time during the visits from those ultra short times which are never long enough for a polytrauma patient.
Yes I know it is my personal medical information I am putting out here, yet my bravery (or stupidity perhaps) to so openly share all this has helped me learn valuable information from others to get properly treated and helped me acquire a higher index of awareness about my body and the care that is or is not given to it.
If you see something here that pertains to something you have questions about maybe I can answer the questions and help in some small way. All in all, recovery and rehabilitation is a work in progress. Not something all diagnosed in an Emergency Room or Ambulance. Things are always unknown or missed there.
Traumatic Brain Injury (approx. one week of amnesia before wreck and 5-6 days after wreck with a few isolated memories in between);
Chronic headaches
head laceration on forehead from just above R brow into hairline approx. 3 inches
moderate right extracranial soft tissue swelling extending to the right periorbital region, paranasal sinus disease with air-fluid levels throughout multiple paranasal sinuses, fluid levels in maxillary area
Whiplash
Multiple teeth fractured, partially missing, or damaged which required numerous oral surgeries to correct through 2014 and 2015
R scapular neck fracture with glenohumeral subluxation
R shattered scapula (comminuted, displaced , and angulated) – [4 surgeries including ORIF and bone grafting]
R 2-11 displaced rib fractures with Flail Chest (ORIF Surgery 5-10 plated); 11th rib still nonunion fracture
R pulmonary contusions, pneumothorax, hemothorax
R lung node (secondary to lung trauma)
T5-10 transverse process nondisplaced fractures, anterior wedging of T6
hairline fracture to right pelvis
R radial styloid fracture
R thigh lacerations status post closure
Multiple soft tissue injuries, seatbelt marks, and scrapes over body
Endocrine Issues (labs all over the place) Amenorrhea 6 months /Irregularity;
MRI of Spine revealed –C3-C4 with central disc protrusion and minor dural sac effacement; C4-C5 some bulging on the disc with mild dural sac effacement, C6-C7 herniated disc with mild to moderate stenosis (focal herniation of the disc posteriorly with generalized bulging, dural sac effacement, and asymmetrical cord flattening on the left); A 15mm hemangioma at T4; T6 wedging/fracture (this remains fractured in 2016 and unhealed); T5-T6, T6-T7,T8-T9 on multiple levels there was disc dessication, loss of disc height, and minimal annular bulge; L4-L5, L5-S1 is a minimal annular bulge, and a Schmorl’s node involving the inferior endplate of L4
Suprascapular Nerve Palsy
Stable 15 cm well-circumscribed nodule posterior inferior of the right thyroid gland, differential includes parathyroid adenoma
Stable subcentimeter thyroid gland nodule and colloid cyst.
Stable noncalcified 5 mm right middle lobe nodule that has been stable for over 2 years
Acromion Fracture (secondary to reconstructive surgery with bone graft and plating to repair)
Anemia persists
Restrictive Ventilatory Defect (2 liters O2 added with CPAP at night)
Posttraumatic Headache
Primary Hypothyroidism with Reverse T3 Syndrome, Secondary Hyperparathyroidism and bowel absorptive problem
Mild to Moderate Hearing Loss Left Ear
Post Trauma Vision Sydrome (PTVS) and Vision Midline Shift Syndrome
Hearing Loss L ear (hearing aid recommended by ENT)
The complexity of Change and how it affects my new normal. I was inspired to write about this for several reasons. I may totally suck at expressing what is in my head here on paper or this screen, but here goes….
It is not all inclusive of every situation in my life, how I see people outside of me in general, how I exist inside myself, or how I handle stress overall in every situation….but it comes pretty darn close to kind of manifesting a picture of an inner struggle that is life as I know it now and my desire to overcome, understand myself, and help others who might experience this after trauma not feel so alone.
I don’t handle “change” as gracefully as I used to. Change in general I have gotten pretty okay with, as a genral rule, if done in advance with plenty of warning or notice (unless it is something time sensitive and important then it is instant anxiety). However I have come to notice that the little stuff…stuff that probably shouldnt even bother me, or wouldnt have before the wreck…does now. Though that can be inconsistent too.
I know…I am consistently inconsistent. Imagine how horrible this inconsistency is for the person going through it who now thrives better with lists, strategies, consistency….or order.
Sometimes last minute changes leave me feeling just gloomy, depressed, and sad. Sad is not my normal emotion with this. Mostly it is being irritated …okay…highly irritable….when things change. Following through the plan has become very important to my daily feeling of a successful day.
I feel I cannot leave the house and feel calm without my to do list (this can be mental or written…though more often it is written). This list will be in a specific order too. If things are done out of order, I get irritated or frustrated and the chance I forget something increases.
Small things/changes that should truly be insignificant in the day that involves me personally, just are not that small to me…they can be monstrously huge in my perception at that time…in that instant.
I cannot explain the sheer anxiety that those little changes cause me now. I used to not mind them so much before the wreck…I would definitely adjust quicker or maybe I just wasn’t aware of them at all…things that just cause hiccoughs throughout a normal day (whether they are small or large). Things that wouldnt slow me down…but now can seemingly paralyze me.
Now though…it is so important to stick to the plan.
If I analyze something afterwards…sometimes I realize it shouldn’t bother me or that I am being ridiculous..or how I should have handled it differently….yet I plan my day based on lists and when those lists change it messes up my day….it throws me off course.
I get that morose feeling when I forget things….it is usually appointments I forget and conversations…important things I am sure I will remember…it is humiliating. I make lots of lists. It kills the mood if I forget them. I am still working on adjusting to that part.
I have come to somewhat have a sense of humor about all this (this depends on what kind of brain day I am having for sure). Some days are better than others.
I recently had someone express it sounded like OCD or impulsivity.
I guess I never recognized it as an OCD thing or being impulsive. I have never had OCD in my life or been diagnosed with that ….maybe it is OCD or not OCD at all. I just know it is inconvenient.
Sometimes if I get all worked up about something (positive or negative), get prepared for it, have all my notes ready, have all the pieces in place and it gets cancelled, or I am late and it gets cancelled, or it ran over and I am late to othet things….that is a real problem for me.
If I am depending on a certain schedule that day and then realize too late that I have looked at the wrong day on the calendar….I sink into embarrassment and self-defeat and dark places inside myself. This can also manifest itself as a sheer and utter sadness, or complete internal rage. I cannot tell you the times I have missed an appointment because I forgot about it (even if I looked at the planner 2-3 hours before that), or the opposite… shown up to an appointment early, proud of myself, to be told I dont have one that day. I have gotten better about checking my planner and my phone to compare dates and times, before arguing with the receptionist. Dealing with the feelings after are another story. Those emotions can very from feeling relief (if I was running late anyway and now get a second chance) to feeling confused and crazy ( if I am really quite sure about the day, the facts, and was feeling confident).
My husband will often accuse me of micromanaging his driving and trying to control his driving and what we do with the day. I assure him that is not it at all or what is going through my head. It is not about HIM. It is about ME. For example, there is a certain way I go to specific places. If he goes a different way it throws me off and then I get anxiety about being late. (I DESPISE being late to anything), or I feel a twinge of irritability that I have to silently or not so silently quell. Also if I gasp or make any sounds at all he is like…”knock it off I’m a good driver Caren when have I ever been in an accident?” I tell him I am and was a good driver too yet accidents still happen. I tell him if something is scary to me. I tell him if something is freaking me out….when things seem enhanced around me and magnified…sometimes just taking an exit ramp can feel like we are tipping over on our side and the wheels have left the ground and enormous fear overwhelms me and I have a deathgrip on whatever I can hold onto and beg him to slow down (even though the wheels dont leave the ground). Even if I look at the speedometer and can “see” we are going an appropriate speed….it feels so different. He doesnt understand that about me now and it has created opportunities for even the kids to get in on comments to mom about whatever is going on or join in on making jokes about it. Other days he can take the same exit faster and it doesnt bother me a bit.
I go one of two ways with anxiety. It is also depending on what kind of a “brain” moment I am in. What I call “enhanced” or “tunnel vision” with my anxiety. Enhanced means that suddenly colors are brighter, lights are brighter, sounds are louder, I notice every movement around us, its intensity in minute ways. This can last moments to all day. Tunnel vision is like when a car is sliding towards me and all I can see is that car and all the peripheral stuff disappears until the car stops sliding. The sliding (whether it is continued or stopped), even if a slight shift in the lane or a flat out across the intersection slide by that car appears greater and larger….it triggers these deep emotions that are just automatic and overwhelming, and often debilitating emotionally, mentally, and sometimes physically. (That is when I feel overstimulated or burst into tears, and it’s time to go home NOW, or an unavoidable nap ensues, .or a meltdown…depending on how intense the situation is).
I then get annoyed or irritable because I am genuinely upset or scared in that moment in the vehicle. I literally feel like something horrific is about to happen or has happened. He tries to joke with me to make me laugh…I have learned to try to go along with that….but sometimes I just start crying instead and not even mean to…then I am mad at myself. It’s not his fault I feel this way. So being mad at him in those moments is not helpful. So I am always analyzing my feelings, my reactions, my words. Sometimes not until after the fact….which can cause some tense moments.
Another example is I am getting ready to leave the house. I have to do things in a certain way now. Okay I think Bag, notebook, pen, planner, phone, charger, wallet, cane, and keys. Sometimes keys comes first but that is the order . Now if one of the kids, or my husband, or anyone, or a phone call interupt that mental walkthrough of the list, and I don’t start the list over…. then I ALWAYS forget something and if its the planner or the phone I am really screwed and it ruins everything about the day if I end up out there without them. I really depend on all those things. Even if I dont use them all on my outing just KNOWING they are with me and functional matters.
Change sometimes comes with complex anxiety. Sometimes it does not. Little things can appear like big things and big things either matter or they don’t. Functioning despite all those nuances is the key. Sometimes finding the right key to all those “locks” is the challenge. I cannot explain it beyond that.
Hello there. I am a polytrauma and TBI survivor. I acquired mine from a wreck (head on collision) where my seatbelt failed and I was ejected (see Frequently Asked Questions page for more details).
I for a long time, felt it wasn’t important to “show” a picture of who I was. I have gotten lots of requests for this though. I realize people want to see a “real” person. I wanted and still want… the site to be something that could be relatable regardless of what a person looks like….because after all…TBI is often invisible. So are most bodily trauma’s once the bones heal. Yet this is NOT the end of the healing process.
This website is a growing passion for me with the more I advocate for myself, learn about myself, and learn about others experiences. This website is an outlet for my continued healing, rehabilitation processes, and a way to share what I have learned with others. Helping One Person Excel I truly believe…begins with who I see in the mirror each day – Me.
To Be Independent is always the goal….yet that comes with a lot of dimensions and levels of intricate obstacles. I hope that you find something in the pages of this site that help you, or someone you know.
If you’d like to share your story, or offer a guest blogging post …that would be amazing. Your story matters. Are you a Survivor, Caregiver, Family Member, Healthcare Provider, Friend, Employer, Co-worker? Whether the person is living or deceased…their story still matters.
Feel free to ask me questions in comments below or in email at hopetbi4ever@gmail.com I will answer as honestly and as directly as possible.
What is a typical day? I used to be able to tell you this until January 4, 2014. That is when everything that became typical about my life, my health, my existence, became consistently ATYPICAL.
I feel like a Turtle walking around in a hollowed out shell moving slowly and hoping I can make it far enough and long enough to get to where it is I am heading. Where is it I am heading? That is a great question. I often forget the answer as I am heading in so many directions at once on so many different levels….even if I am sitting perfectly still and quiet.
HOPE can only get you so far. I try to hold myself back from the dark abyss of resentment and emotion that try to pull me over that cliff of depression that reminds me of all my limitations, injuries, pain, and I feel robbed. I am robbed not only of my function, endurance, memories, peace, and joy. I feel robbed of opportunities, freedoms, laughter, and just simple existence.
I guess all my new normals that are no longer really new….yet new enough to feel like fresh wounds with salt dripped into them on a daily basis are who I am now.
I wake up sometimes more tired than when I went to bed. Sometimes I wake up ready to conquer the world only to be exhausted by the time I muster enough energy to actually get dressed or to take a shower. Then other days I am blessed with a full day of accomplishment. I actually get out of the house and make my way through the world ignoring all the struggles that seek to slow me down (pain, confusion, forgetfulness, dashed joy, excitement, fatigue, bathroom breaks, sadness, and the seeming lack of motivation for life all at the same time).
What is a typical day? The only typical day is that I know I will face…..is a mountain of uncertainty. Will I have an accident? Will I forget something important? Will I be late? Will I remember to use my words and respond instead of just reacting emotionally? Will I get everything done I have put on the list? Where is the list? Did I make a list? Where is my planner? Where is my phone? Where is my charger? Where are my shoes? okay let’s go….oh crap, I forgot to put on pants. Okay pants on now…wait where did I put my bag. Do I have my planner, my phone, a pen? My charger….wait…gotta pee…okay flush toilet wash hands phone rings get planner talk on phone …kids talking “mom mom mom” wave them away finish on phone….head spinning I have everything right? Feeling irritable already. Oh no I read the time wrong now I am super late. I totally need help here feel like I am drowning. Feeling flooded and overwhelmed or not just yet but feel it coming on. Try to avoid it. Deep breathing, Relax. Husband asks if he can help or he doesnt ….kids a distraction or they aren’t. Okay let’s go…wait I need to have water with me. Man am I thirsty. I have to remember to take my meds. Okay do I need meds now? What is my pain level? Lets skip pain meds I can do it. Oh my gosh what was I thinking? I have to be somewhere but I can’t put my finger on it. What was I doing? Where am I going…I don’t remember. I look at the white dry erase board what is today? I cannot remember what day it is. Look at phone. OH okay…I have it now. Oh no I got my days wrong I don’t have appointment today….wait yes I do I looked at the wrong day. Okay lets go. What am I forgetting? It feels like I am forgetting something. Where’s my list of questions for the provider? Where is my List I know I had a list….oh that’s right I forgot to do the list because I fell asleep. Okay out the door, let’s go. Get in van, let’s go…. pat pockets for phone; crap – muscle spasm; damn this headache, I will be fine. I feel like vomiting. I am a passenger n vehicle and moving now….crap I left my bag at home with my planner. Panic what do I do? Focus, look at phone distract yourself. You are safe. It’s okay. No planner can’t go back or will be late. Have to have planner MUST have planner. Panic ensues or it doesn’t. Go get planner or skip it if running behind which is often even if ready to go early. Leave without planner day ruined. If leave without phone feel lost and alone day ruined. I have alarm reminders and email and ways to communicate with people if I need help with something. In vehicle “no don’t hit us” *car swerves in our lane or slams on their brakes or gets too close to us”. Oh my gosh I cannot wait to get home. Okay I can do this. Quit wimping out Caren push push push. You can do it. Not so bad right….oh crap another muscle spasm. I am really hurting today or not really hurting as much. I am happy but so worn out and I haven’t even done anything yet; or I feel great and then someone zooms in front of us or we see someone almost wreck or act crazy…instant fear and nap time to escape brain shuts down I am done. NO! I have too much to do. NO sleeping. I am sorry I didn’t mean to fall asleep. Are we there yet? Thank God I did it. I knew I could do it. Why can’t I get anything right? I hate forgetting so much. Slow down. I want to go home. I feel like crying every little sound is annoying. Talking is annoying, the wind when the windows are down is annoying. Man my back hurts, my neck is killing me. Wow my shoulder feels better since surgery now…I love those people. I think I am going to cry I am so happy my shoulder is getting better. Oh my gosh how will I get through this day. I am already running low on energy. Wait…where’s the bathroom. I have to go RIGHT NOW….great a piddle I hope noone can tell. Did I bring extra underwear? Oh yes I did…. get relief or no I didn’t shame lingers. Good morning world I love you or I can’t stand any of you at this moment and I don’t know why. Shhhhhhh not so loud the lights hurt my eyes. I am okay. What? You want me to answer what question? Yes I am okay. Why are you staring. I don’t care if you stare I am proud to be alive or man I can’t get away from the pain to I just can’t stay awake I am sorry I AM DONE…my brain is done. Can we go home now? Think Think Think what was I doing? Oh That’s right, smile act normal. Stay quiet or not so much. Wash rinse repeat every day.
Some days are a blessing. Calm quiet, no appointments, no need to think, no need to go anywhere or do anything. Time to sleep to recover from the days I was just existing.
So I focus as much as I can on researching myself learning about how to get my quality of life back leaving no stone unturned. Yet some days defeat wins a round and I cannot even get out of bed to get dressed. Sometimes I am hurting so bad the tears flow and I cannot stop them hard as I might.
I feel defensive like I have to try and explain why I am late, moving slowly, hurting, forgetful, struggling in some parts of my day and not others, yet there is nothing to defend. I feel like I have to explain everything as I go to educate others when they just don’t understand. That is not my job. What is a short answer? I don’t even know really anymore. So I just say it’s a good day to be alive.
I detest being late. I detest even more forgetting things. Important things. Conversations, appointments, easy things, important things. Why can I remember some things and not others. Why are there so many gaps. It is what it is I keep telling myself. Apply your strategies Caren. I can be vicious with my words and equally as generous. I can be brave and fierce and face the pain or I can crumble like a wadded up piece of paper. The only thing that is consistent is my inconsistencies.
No, it’s not fair, it’s not productive, it’s not ideal. It’s not easy. Yet it is an opportunity to appreciate life in a different way and I am constantly caught between never giving up hope and just not giving a crap anymore. Sometimes the fight to recovery is just so painful and long and lonely and utterly draining. Sometimes you just feel like damaged goods overwhelmed by trying to not forget all the things that are important to make it through each day. Sometimes each moment. Then it passes and all is well with the world again…for just a little while. I talk yet noone hears me. I listen but their mouth moves and I don’t hear their words. Never the same. Nothing can explain it. A different language or no talking at all.
The journey on these dusty roads are not without exhaustive effort. Hard as you try to keep from getting dirty you are bound to have accidents, forget important things and be late to things. If there is one lesson to be learned in all of this – it is to face your fears and do not let them eat you alive. Forgive yourself for forgetting and remember that you know you better than anyone else. Sometimes invisible effort. Sometimes invisible limitations. Sometimes invisible pain is more painful than the fractures that resist healing and like those fractures need added support. My goal is to pave those dusty roads with healthy recovery and continue to use tools to survive with. I am not stupid by far, just different than what I once was. So I will mosey on along like the turtle….. slow…. to control the pain and thrashing muscle groups. Slow so I respond and not react. Slow so I can gather my thoughts. Slow so I can hold on to what I need and release what is not effective. Slow and steady wins the race. Isn’t that the ending?
Damaged goods? I say yes. Destroyed? I say no. Fight or flight? Let’s get those wings!
Well. Do we have a LOT to catch up on. No I haven’t dropped off the face of the Earth somewhere. Though some days I do feel quite invisible…but that is another post entirely. Trying to keep things real and authentic here and in my mind I have written each update a million times and nothing I felt I could say here matched what was in my head. So tonight, I was just like….well…to heck with it – just be out there with it.
We miraculously by the skin of out teeth made it to MN. We still have not been properly or fully reimbursed for our January, February, or March trip. This has been financially debilitating to us, however, that is not what I want this blog to be focused on.
What I do want to keep the focus on – is the progress and new medical developments that I have encountered, am learning about, and am hoping may help one of you out there in some way. Perhaps someone you even know or have known or will know at some point and time.
So I admittedly have been depressed. On February 5, 2016 I had a PT appt at home. I then had a PCP appt after that. Well, my husband was helping me get dressed, like he has done so many times before. I laid my arm on his arm so he could help get my shirt on me and we heard the loudest POP or CRACK I have heard from a body part. It instantly shot pain up the side of my neck and to my ear. Then strings of pain across my R chest and into my back some. It was dreadful. I couldn’t put my arm down and the pain was IMMENSE. At my PCP’s office she checked me out and reasoned with me that since it “felt” palpably okay that it was most likely recovery pain. I told her it didn’t feel right. I had even called MN that same day on the way to her office to leave a message for Dr. Cole (my orthopedic surgeon). It was on a Friday and since we were going to be in MN on that next week my PCP opted not to xray it.
Well we went…and bottom line is that POP was a BONE being FRACTURED…..a horrible sound I might add. I had apparently fractured my Acromion process (top of my shoulder). Now based on what Dr. Cole explained this was rare (from what we read with our online research – only like 7%- (of course this is rare I thought). He had an xray and CT done. I will say that I have come to realize that xrays have not been incredibly diagnostic for me all along. For some they are better and some they aren’t – me well not so much.
So what did that mean. Well it was aligned for now and I had to do absolutely nothing with it until my next appointment in March to hopefully give it time to heal. Start the protocol all over as if I had just gotten out of surgery. I will say the pain was horrible….but different than shattered pain. I would also say that I am being very well acquainted with a multitude of pain experiences and each have their own level of challenges and differences. How I moved before the scapula surgery that would give me some relief here and there did NOT work for this fracture. I was petrified for it to get separated. If it did get misaligned that would mean potential surgery…This time on the Acromion. We were super super cautious and eventually the neck pain, chest pain and such receeded back into the center of the top of my shoulder to remind me just how broken it was OUCH. But hey… progress is progress. Oh and PT and OT got put on hold. NO Chance of geting that misaligned.
It was a LONNNNNNNNG several weeks. We saw Dr. Cole again on March 16th and this is where we learned That gosh darn fracture hadn’t healed yet and was separated a bit…not by much and he debated just going in to get it repaired and plated while I was there, however it did show bone growth, even though still quite painful and limiting. My head of course was swimming with information and questions that I didin’t seem to be able to get out the way I wanted – so I just listened – not really getting it yet. He decided to cancel the April appointment and then set an appointment for May 2016 to give the body time to do what it appeared to be doing ever so slowly – trying to heal itself. That meant however, no weight bearing at all with my right arm though I could begin again with PT conservatively.
So in May we find out whether I stay for a bit to plate this bad boy and fix it for good, or whether nature has taken its time, but actually healed it properly. That appointment feels like its lightyears away.
There is actually some awesomely good news in all of this though. There is a LOT less pain in my scapula. Like it is miraculous how much he helped me with those January surgeries so I have utter faith in this man – even if I do have to have another surgery I know….like truly know he will make it better.
I am still quite limited but that will just take time and lots of therapy to get my strength back up. We don’t know how much of the nerve damage will remain, continue to affect things, and all that stuff. Time will tell. I will say that it just flooded me like
REALLY MORE BROKEN STUFF!!!! It was a lot to absorb and focus on in a positive way. After a while, even though I know things were feeling different in some ways and better…..they were worse in other ways and status quo in yet other ways. Also fighting with Insurance to get basic quality of life and such should not be a constant fight and battle. This just adds to the stress and I truly believe slows the healing process because now you are always focused on that next ball getting dropped by them….it’s distracting, annoying, and is something that needs reformed for sure. That’s my soapbox on that though.
So here we go. Working hard to stay afloat. Not just financially but in the dynamics of our relationships with each other in the house. The trips are hard on my body and my brain. I think I am going to end up with the back pain for life. The headaches are crazy consistently unrelenting and so mch a part of me now that I don’t remember when I last never had one.
I feel so flooded and overwhelmed after I get home fro travelling that I literally crash out and sleep like I haven’t had sleep in days. Going each way usually takes me a few days to play catch up with my already seemingly dulled self. There is so MUCH stimulation that I was never aware that I was aware of before. Travelling def makes a difference. I have totally decided that travelling by train is much less intense than by Plane. Still tons of people and still tons of noise and activity, but we get our own room which helps quite a bit with trying to get a grip…..and it is way more economical.
We keep moving forward….making impossible choices….going with the flow Time and time again. The future uncertain, but glad that I am still here to have a future to be uncertain about…..
So sorry for the delayed update – more posts to come…..just been battling exhaustion, pain, fatigue, and a good dose of BLAH!
This Website is a gift of love. To myself, to my husband, to my mom, my children, and all those that have been touched by trauma in any form. To those who have cared for me or tended to me in any way, I continue to learn something from each person I come into contact with. Even those I may not readily remember.
When I came home from the hospital….my body was home, but not all of me….not really. I am getting to learn the “new” me, while remembering the me I used to be. Welcome to a glimpse into the world of having a TBI (Traumatic Brain Injury) among other things. The steps in this tumultuous journey I will share with you in these pages, as time goes on. Thank you for reading this blog. Welcome. Come on in, stay a while.







































































 numbers). Hang somewhere visible, so it can be seen and utilized daily. Update the same day weekly or as schedules change.
numbers). Hang somewhere visible, so it can be seen and utilized daily. Update the same day weekly or as schedules change.
 If something changes in the schedule, write it down IN THE PLANNER. Label cupboards and storage containers as a reminder of where things are kept; label doors as a reminder of which room is which.
If something changes in the schedule, write it down IN THE PLANNER. Label cupboards and storage containers as a reminder of where things are kept; label doors as a reminder of which room is which. Use post-it/sticky notes. You can use them anywhere in your home or personal workspace to remind you to do specific tasks (such as a sticky on a library book that has to be returned by a certain date, or start load of laundry today, etc).Once you have completed the task, it’s important to throw the post-it/sticky note away. This way you won’t accidentally redo what you already finished.
Use post-it/sticky notes. You can use them anywhere in your home or personal workspace to remind you to do specific tasks (such as a sticky on a library book that has to be returned by a certain date, or start load of laundry today, etc).Once you have completed the task, it’s important to throw the post-it/sticky note away. This way you won’t accidentally redo what you already finished. some can be set to remind you when to take your pills, with an alarm, vibration or flashing light.
some can be set to remind you when to take your pills, with an alarm, vibration or flashing light. n), all medications and their dosages (remember to list any herbs, supplements taking), and list of concerns. Record meetings or appointments to go back and listen to later and take notes from the recording.
n), all medications and their dosages (remember to list any herbs, supplements taking), and list of concerns. Record meetings or appointments to go back and listen to later and take notes from the recording.








 Keep in mind when talking about that “elephant in the room” that sometimes the very people who need to hear the topic being talked about are the least receptive to hearing it. That often means that person might even be you. Being receptive to talk is important. It is equally as important to actively listen. Support from others that share the same or differing opinions about the issues you wish to speak about will make it not about you, but about the issue and how much it impacts others who have gone through the same thing, or are currently experiencing the same challenges. Support groups (even if they are online) can be an amazing source of support, ideas, and encouragement.
Keep in mind when talking about that “elephant in the room” that sometimes the very people who need to hear the topic being talked about are the least receptive to hearing it. That often means that person might even be you. Being receptive to talk is important. It is equally as important to actively listen. Support from others that share the same or differing opinions about the issues you wish to speak about will make it not about you, but about the issue and how much it impacts others who have gone through the same thing, or are currently experiencing the same challenges. Support groups (even if they are online) can be an amazing source of support, ideas, and encouragement.








 In the beginning I was at the point when I couldn’t easily reset myself, so I would say “BRAIN TIME”, go in my room (or they would have to leave my room), and I would stay there until things settled down in my head. No interruptions, no calls, no questions, door shut. Sometimes this was moments, sometimes minutes, often hours, or occasionally days. I needed absolute silence, a dark room, a warm heavy blanket and to lay down perfectly still. I slept a TON.
In the beginning I was at the point when I couldn’t easily reset myself, so I would say “BRAIN TIME”, go in my room (or they would have to leave my room), and I would stay there until things settled down in my head. No interruptions, no calls, no questions, door shut. Sometimes this was moments, sometimes minutes, often hours, or occasionally days. I needed absolute silence, a dark room, a warm heavy blanket and to lay down perfectly still. I slept a TON. Two and a half years after the trauma I started to return to driving. I would learn my inner compass was missing/broken. I was horrified to find myself LOST after taking my kids to school. In fact, I couldn’t remember how to get there….a trip I had made hundreds of times before. I used a GPS because it was like I had never been there before. Now THAT made me feel coo-koo….I didn’t understand. Then I got lost heading home. I literally ended up 20 minutes in the opposite direction because I couldn’t remember what to do or how to get where I needed. GPS became an absolute crutch. As time has gone on, I have gotten better about figuring out my routes. Often times I could think of where I needed to go…yet applying it to real life outside my head was a different reality entirely.
Two and a half years after the trauma I started to return to driving. I would learn my inner compass was missing/broken. I was horrified to find myself LOST after taking my kids to school. In fact, I couldn’t remember how to get there….a trip I had made hundreds of times before. I used a GPS because it was like I had never been there before. Now THAT made me feel coo-koo….I didn’t understand. Then I got lost heading home. I literally ended up 20 minutes in the opposite direction because I couldn’t remember what to do or how to get where I needed. GPS became an absolute crutch. As time has gone on, I have gotten better about figuring out my routes. Often times I could think of where I needed to go…yet applying it to real life outside my head was a different reality entirely. If they turned their backs to me I would ask them to turn around and repeat what they said. Some folks are super accommodating, some act put out by this. Often times folks think you aren’t interested in listening or you do not care about what they said. It wasn’t that, I just couldn’t process what they were saying. Sometimes the words didn’t make sense. It’s like I was listening to a foreign language sometimes. Sometimes it was like I could see their mouth moving, hear noise coming out, yet couldn’t make out the words. This was maddening. Oh! if I was doing something and all my focus was on it (like typing or reading), forget about me hearing you..it just didn’t happen.
If they turned their backs to me I would ask them to turn around and repeat what they said. Some folks are super accommodating, some act put out by this. Often times folks think you aren’t interested in listening or you do not care about what they said. It wasn’t that, I just couldn’t process what they were saying. Sometimes the words didn’t make sense. It’s like I was listening to a foreign language sometimes. Sometimes it was like I could see their mouth moving, hear noise coming out, yet couldn’t make out the words. This was maddening. Oh! if I was doing something and all my focus was on it (like typing or reading), forget about me hearing you..it just didn’t happen. After the polytrauma I seemed to lose the ability to feel hunger or fullness. For some bizarre and I am sure possibly scientific reason I lost my appetite or desire for food in general. No more interests, no more favorites, no more “cravings”, and no more enjoying the things I used to enjoy before. My sense of taste and smell had changed. Some of the things I enjoyed before now repulsed me. Smelling certain types of food cooking was enough to turn me “green” (sick). Just looking at certain types of food was repulsive. The connection with food emotionally seemed to go on vacation. In fact, if I wasn’t brought my meals in those early months and sometimes still…I just wouldn’t eat because I would just forget to eat or have no interest in it.
After the polytrauma I seemed to lose the ability to feel hunger or fullness. For some bizarre and I am sure possibly scientific reason I lost my appetite or desire for food in general. No more interests, no more favorites, no more “cravings”, and no more enjoying the things I used to enjoy before. My sense of taste and smell had changed. Some of the things I enjoyed before now repulsed me. Smelling certain types of food cooking was enough to turn me “green” (sick). Just looking at certain types of food was repulsive. The connection with food emotionally seemed to go on vacation. In fact, if I wasn’t brought my meals in those early months and sometimes still…I just wouldn’t eat because I would just forget to eat or have no interest in it. I have come to realize that my thyroid-pituitary-hypothalmus axis was way off. My hormones were all over the place and apparently I rattled that temperature control center of my brain pretty good.
I have come to realize that my thyroid-pituitary-hypothalmus axis was way off. My hormones were all over the place and apparently I rattled that temperature control center of my brain pretty good.






 brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.
brain inflammation or swelling. This can lead to restricted blood supply to the brain tissue and brain herniation. Tonsillar herniation is a type of cerebral herniation characterized by the inferior descent of the cerebellar tonsils below the foramen magnum. Chiari one malformation is a form of tonsillar herniation and is now known to be caused by trauma (like severe whiplash and traumatic brain injury) or in most cases “symptoms awakened” from trauma. This is an often overlooked correlation between trauma and DAI and TBI.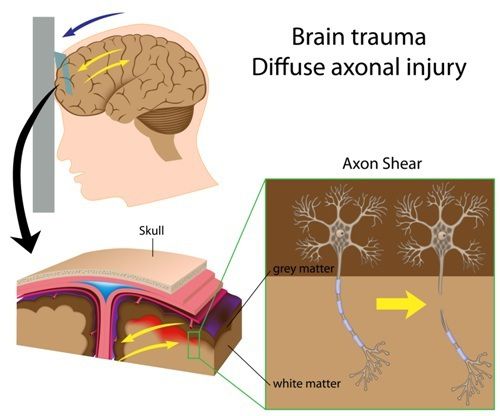 PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage.
PTA is another good estimate for severity of a brain injury. Anytime a person has a major blow to the head he or she will not remember the injury and related events for some time afterward. People with these injuries might not recall having spoken to someone just a couple of hours ago and may repeat things they have already said. This is the period of posttraumatic amnesia. The longer the duration of amnesia, the more severe the brain damage. Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.
Also, more intelligent people may enjoy higher processing speed or impulse conduction in brain-wires (axons). But with more complexity in the brain, the net result still could look in performances as much slower decision making resulting in a dulled sense of self, lower test scores compared with their education/experiences, and reduced overall performance compared with their performance before injury.

 not own it as my own, but rather something I experienced.
not own it as my own, but rather something I experienced. may be thinking wow thanks for sharing information I didn’t need to know. Why does this matter to me as a reader? Good question!!!
may be thinking wow thanks for sharing information I didn’t need to know. Why does this matter to me as a reader? Good question!!!




 You are safe. It’s okay. No planner can’t go back or will be late. Have to have planner MUST have planner. Panic ensues or it doesn’t. Go get planner or skip it if running behind which is often even if ready to go early. Leave without planner day ruined. If leave without phone feel lost and alone day ruined. I have alarm reminders and email and ways to communicate with people if I need help with something. In vehicle “no don’t hit us” *car swerves in our lane or slams on their brakes or gets too close to us”. Oh my gosh I cannot wait to get home. Okay I can do this. Quit wimping out Caren push push push. You can do it. Not so bad right….oh crap another muscle spasm. I am really hurting today or not really hurting as much. I am happy but so worn out and I haven’t even done anything yet; or I feel great and then someone zooms in front of us or we see someone almost wreck or act crazy…instant fear and nap time to escape brain shuts down I am done. NO! I have too much to do. NO sleeping. I am sorry I didn’t mean to fall asleep. Are we there yet? Thank God I did it. I knew I could do it. Why can’t I get anything right? I hate forgetting so much. Slow down. I want to go home. I feel like crying every little sound is annoying. Talking is annoying, the wind when the windows are down is annoying. Man my back hurts, my neck is killing me. Wow my shoulder feels better since surgery now…I love those people. I think I am going to cry I am so happy my shoulder is getting better. Oh my gosh how will I get through this day. I am already running low on energy. Wait…where’s the bathroom. I have to go RIGHT NOW….great a piddle I hope noone can tell. Did I bring extra underwear? Oh yes I did…. get relief or no I didn’t shame lingers. Good morning world I love you or I can’t stand any of you at this moment and I don’t know why. Shhhhhhh not so loud the lights hurt my eyes. I am okay. What? You want me to answer what question? Yes I am okay. Why are you staring. I don’t care if you stare I am proud to be alive or man I can’t get away from the pain to I just can’t stay awake I am sorry I AM DONE…my brain is done. Can we go home now? Think Think Think what was I doing? Oh That’s right, smile act normal. Stay quiet or not so much. Wash rinse repeat every day.
You are safe. It’s okay. No planner can’t go back or will be late. Have to have planner MUST have planner. Panic ensues or it doesn’t. Go get planner or skip it if running behind which is often even if ready to go early. Leave without planner day ruined. If leave without phone feel lost and alone day ruined. I have alarm reminders and email and ways to communicate with people if I need help with something. In vehicle “no don’t hit us” *car swerves in our lane or slams on their brakes or gets too close to us”. Oh my gosh I cannot wait to get home. Okay I can do this. Quit wimping out Caren push push push. You can do it. Not so bad right….oh crap another muscle spasm. I am really hurting today or not really hurting as much. I am happy but so worn out and I haven’t even done anything yet; or I feel great and then someone zooms in front of us or we see someone almost wreck or act crazy…instant fear and nap time to escape brain shuts down I am done. NO! I have too much to do. NO sleeping. I am sorry I didn’t mean to fall asleep. Are we there yet? Thank God I did it. I knew I could do it. Why can’t I get anything right? I hate forgetting so much. Slow down. I want to go home. I feel like crying every little sound is annoying. Talking is annoying, the wind when the windows are down is annoying. Man my back hurts, my neck is killing me. Wow my shoulder feels better since surgery now…I love those people. I think I am going to cry I am so happy my shoulder is getting better. Oh my gosh how will I get through this day. I am already running low on energy. Wait…where’s the bathroom. I have to go RIGHT NOW….great a piddle I hope noone can tell. Did I bring extra underwear? Oh yes I did…. get relief or no I didn’t shame lingers. Good morning world I love you or I can’t stand any of you at this moment and I don’t know why. Shhhhhhh not so loud the lights hurt my eyes. I am okay. What? You want me to answer what question? Yes I am okay. Why are you staring. I don’t care if you stare I am proud to be alive or man I can’t get away from the pain to I just can’t stay awake I am sorry I AM DONE…my brain is done. Can we go home now? Think Think Think what was I doing? Oh That’s right, smile act normal. Stay quiet or not so much. Wash rinse repeat every day. So I focus as much as I can on researching myself learning about how to get my quality of life back leaving no stone unturned. Yet some days defeat wins a round and I cannot even get out of bed to get dressed. Sometimes I am hurting so bad the tears flow and I cannot stop them hard as I might.
So I focus as much as I can on researching myself learning about how to get my quality of life back leaving no stone unturned. Yet some days defeat wins a round and I cannot even get out of bed to get dressed. Sometimes I am hurting so bad the tears flow and I cannot stop them hard as I might. from getting dirty you are bound to have accidents, forget important things and be late to things. If there is one lesson to be learned in all of this – it is to face your fears and do not let them eat you alive. Forgive yourself for forgetting and remember that you know you better than anyone else. Sometimes invisible effort. Sometimes invisible limitations. Sometimes invisible pain is more painful than the fractures that resist healing and like those fractures need added support. My goal is to pave those dusty roads with healthy recovery and continue to use tools to survive with. I am not stupid by far, just different than what I once was. So I will mosey on along like the turtle….. slow…. to control the pain and thrashing muscle groups. Slow so I respond and not react. Slow so I can gather my thoughts. Slow so I can hold on to what I need and release what is not effective. Slow and steady wins the race. Isn’t that the ending?
from getting dirty you are bound to have accidents, forget important things and be late to things. If there is one lesson to be learned in all of this – it is to face your fears and do not let them eat you alive. Forgive yourself for forgetting and remember that you know you better than anyone else. Sometimes invisible effort. Sometimes invisible limitations. Sometimes invisible pain is more painful than the fractures that resist healing and like those fractures need added support. My goal is to pave those dusty roads with healthy recovery and continue to use tools to survive with. I am not stupid by far, just different than what I once was. So I will mosey on along like the turtle….. slow…. to control the pain and thrashing muscle groups. Slow so I respond and not react. Slow so I can gather my thoughts. Slow so I can hold on to what I need and release what is not effective. Slow and steady wins the race. Isn’t that the ending?